I was recently invited to visit an academic anesthesiology department to speak to the residents about becoming a leader (see SlideShare). In addition to recognizing the honor and privilege of addressing this important topic with the next generation of physician anesthesiologists, I had two other initial thoughts: 1) I must be getting old; and 2) This isn’t going to be easy.
I came up with a short list of lessons that I’ve learned over the years. While some examples I included are anesthesiology-specific, the lessons themselves are not. Please feel free to edit, adapt, and add to this list; then disseminate it to the future physician leaders who will one day take our places.
First and foremost, be a good doctor. Always remember that we as physicians take an oath. In the modern version of the Hippocratic Oath commonly recited at medical school graduations today, we say, “May I always act so as to preserve the finest traditions of my calling and may I long experience the joy of healing those who seek my help.” As a physician anesthesiologist, we care for the most vulnerable of patients—those who under anesthesia cannot care for themselves. Examples of anesthesiologists who do not honor their calling exist in the news and even scientific journals, but we cannot follow this path.
Define your identity. We live in the era of the “provider,” and this sometimes causes role confusion from the perspective of our patients. We also don’t tend to do ourselves any favors. How many times have you heard someone say, “Hi I’m [first name only] with anesthesia”? According to the American Society of Anesthesiologists newsletter, approximately 60% of the public may not know that physician anesthesiologists go to medical school. While every member of the anesthesia care team plays a crucial role, the next level of non-physician provider in this model has one-tenth the amount of clinical training when compared to a physician anesthesiologist at graduation. I’ve written before about what I love about being an anesthesiologist, and being the physician whom patients trust to keep them safe during surgery is a privilege which comes with a great deal of responsibility.
Consider the “big picture.” The health care enterprise is constantly evolving. Today, the emphasis is on value and not volume. Value takes into account quality and cost with the highest quality care at the lowest cost being the ultimate goal. The private practice model of anesthesiology has changed dramatically in the last few years with the growth of “mega-groups” created by vertical and horizontal integration of smaller practices and sometimes purchased by private investors. In this environment, physician anesthesiologists and anesthesiology groups will have to consider ways they can add value, improve the patient experience, and reduce costs of care in order to stay relevant and competitive.
Promote positive change. Observe, ask questions, hypothesize solutions, collect data, evaluate results, draw conclusions, and form new hypotheses—these are all elements of the scientific method and clinical medicine. These steps are also common to process improvement, making physicians perfectly capable of system redesign. The key is establishing your team’s mission and vision, strategic planning and goal-setting, and regularly evaluating progress. Books have been written on these subjects, so I can’t do these topics justice here. In my opinion, physicians offer an important and necessary perspective that cannot be lost as healthcare becomes more and more business-like.
Be open to opportunities. Thomas Edison said, “Opportunity is missed by most people because it is dressed in overalls and looks like work.” I have written previously about the merits of saying yes. As a resident or new staff physician, it often seems impossible to get involved. However, most hospital committee meetings are open to guests. Consider going to one that covers a topic of interest and volunteer for a task if the opportunity presents itself. In addition, many professional societies invite members to self-nominate for committees or submit proposals for educational activities at their annual meetings.
Thank your team. Taking the first steps on the path to leadership is not going to be easy. There will be many obstacles, not the least of which is time management. A high-functioning healthcare team of diverse backgrounds, skills, and abilities will accomplish much more than what an individual can do alone. Celebrate team wins. Respect each team member’s opinion even when it differs from yours.
I am a physician, clinical researcher, and educator.
I am also on Twitter and tweet under the handle @EMARIANOMD.
Naturally you may ask: “How does Twitter fit into a physician’s academic career?” Some of the benefits that Twitter offers doctors have been described previously by Dr. Brian Secemsky and Dr. Marjorie Stiegler among others. Here are a few reasons of my own:
Global Interaction: Through Twitter I interact with people from around the world with similar interests. Participating in Twitter chats like #healthxph or #hcldr can foster innovative ideas that may lead to research questions or other educational opportunities. For example, by tweeting on #kneereplacement, I was invited by orthopedic surgeon, Dr. Brian Hatten, to revise the anesthesia information page on his site, My Knee Guide, an incredible online portal for people considering or undergoing knee replacement surgery.
Search Optimization: On multiple occasions, I have found research articles that my traditional PubMed searches have missed through the tweets posted by colleagues. I have even been able to relocate certain articles faster on Twitter than PubMed when I know they have been tweeted. Researchers can think of hashtags (starting with “#”) essentially like keywords in the academic world. I periodically check #anesthesia, #meded, #pain, and #kneereplacement for new articles related to my research interests.
Lifelong Learning: When I was in training, I used to peruse the pages of JAMA and New England Journal of Medicine (NEJM) in addition to my own specialty’s journals. Today, it’s difficult to even keep up with new articles just in my own subspecialty. Now I follow JAMA and NEJM on Twitter. By following journals, professional societies, and colleagues with similar interests, I honestly feel that my breadth of knowledge has increased beyond what I would have acquired on my own.
Research Promotion: As a clinical researcher, my hope is that my study results will ultimately affect the care of patients. Sadly, the majority of traditionally-published scientific articles will not be read by anyone besides the authors and reviewers. Through Twitter, I can alert my followers when our research group publishes an article. I also get feedback and “peer review” from colleagues around the world. After a recent publication that I tweeted, I received comments from anesthesiologists in Canada and Europe within an hour!
Enriched Conference Experience: A growing trend at medical conferences is “live-tweeting” the meeting. One of my own issues when I attend or present at conferences is that I feel like I miss much of the meeting due to scheduling conflicts. By living vicariously through my colleagues’ tweets at #ASRASpring15 for example, I can pick up pearls of wisdom from speakers in other sessions even while sitting in a different hall. I can also “virtually” attend conferences by following tweets under the hashtags of meetings like #PCP15 in the Philippines in the comfort of my own home.
I often get asked: “Does anyone really care if I tweet what I eat for breakfast?” Probably not. The truth is that you don’t have to tweet anything at all if you don’t want to. Up to 44% of Twitter accounts have never sent a tweet. Of course, to be a physician actively engaged on Twitter requires respect for patient privacy and professionalism. I recommend following Dr. John Mandrola’s 10 rules for doctors on social media.
In an interview during Stanford’s Big Data in Biomedicine Conference (video below), I had a chance to explain why I tweet. I’ll admit that getting started is intimidating, but I encourage you to try it if you haven’t already. I promise that you won’t regret it, and chances are that you’ll be very happy you did. If you’re still too worried to take the leap, I suggest reading these tips from Marie Ennis-O’Connor to boost your confidence. At least sign up, reserve your handle, and observe.
Observation is still a key part of the scientific method.
Inscribed on a plaque just below a statue of an eagle in front of my hospital is a famous quote from President Abraham Lincoln that begins, “To care for him who shall have borne the battle….”
It is the reason why the Veterans Affairs (VA) system exists. It is the reason why we VA physicians come to work each day.
I am honored to care for our special patient population, and I admit to getting defensive when I hear negative, sensationalistic news about the VA. In truth, VA physicians have good reasons to take pride in their health care system and should be inspired to take on leadership roles.
In 1994, the VA was by far the largest networked health care system in the US. It consisted of 172 acute care hospitals, 350 hospital-based outpatient clinics, 206 counseling facilities, and 39 residential care facilities, with a budget of over $16 billion annually, and was “highly dysfunctional” according to an article co-authored by Kenneth W. Kizer, MD, MPH, the former Under Secretary of Health under President Clinton who headed the VA health care system from 1995-1999.
A decade later, the VA had turned around dramatically. When Philip Longman, a writer with a long interest in health policy, looked for potential solutions to the healthcare crisis in the United States, he found his “muse” within the VA—not in the private sector. He titled his 2007 book about the VA health care system: Best Care Anywhere: Why VA Health Care is Better Than Yours. What happened to make the VA go from worst to first?
In the mid-1990s, Dr. Kizer guided the VA to reset its focus on three core missions:
Providing medical care to eligible veterans to improve their health and functionality
Educating healthcare professionals
Conducting research to improve veteran care.
His strategies led to a dramatic transformation that took less than five years. VA health care showed a statistically-significant improvement in all quality of care indicators after the reengineering when compared to the same indicators before, and these improvements were evident within the first two years. By 2000, the VA outperformed Medicare hospitals on 12 of 13 quality of care indicators. A comprehensive study using RAND Quality Assessment Tools showed that VA adherence to recommended processes of care exceeded a comparable national sample. In terms of surgical care, the VA matched or outperformed non-VA programs in rates of morbidity and mortality.
Integral to this transformation was a remarkable nationwide rollout of an electronic health record in less than three years, with the last facility going live in 1999, long before most health care systems in the United States had even started. Other notable achievements during this period of reengineering included:
350,000 fewer inpatient admissions (FY 1999 vs. FY 1995) despite a 24% increase in patients treated overall;
A decrease in per-patient expenditures by 25%;
An increase in proportion of surgeries performed on an ambulatory basis (80% in FY 1999 vs. 35% in FY 1995);
A 10% increase in total number of surgeries performed with a decrease in 30-day morbidity and mortality;
VA health user satisfaction scores that exceeded the private sector; and
Realignment of the VA medical research program with establishment of a new translational research program, the Quality Enhancement Research Initiative (QUERI).
These achievements were not the result of one person’s efforts. Change implementation required engagement of front line staff, especially the physicians and other health care providers. Unfortunately last year’s VA waitlist scandal raised serious concerns related to veterans’ access to care, scheduling practices, and the reporting of performance metrics. In an article published in the New England Journal of Medicine, Dr. Kizer expressed his concerns regarding variability in the quality of care provided within VA in 2014 when compared to other top-tier integrated healthcare systems. Some VA hospitals performed remarkably well while others did not, and some facilities severely lacked personnel and resources.
Today, there are approximately 9 million veterans enrolled in VA health care, and the VA needs physicians to step up and be leaders. Advanced technology (e.g., secure messaging, e-consultation, and clinical video telehealth) already exists within the VA to streamline communication between patients and physicians and can be used to promote patient-centered, personalized health care and improve access. Some of the highest impact medical research in the world takes place within VA, performed by VA physician scientists, and requires leaders to advocate for continued funding. The results of these studies and others should form the basis of best clinical practices that VA physician leaders need to disseminate and implement at their respective facilities. VA physicians have pioneered the field of simulation education, and this represents one tool that may be used to facilitate dissemination. The VA has arguably the richest and most mature electronic health record in the country, if not the world; yet these data are not easily accessible. Physicians on the front lines of patient care, those engaged in research, and those in leadership positions need to advocate for resources to develop real-time analytics and harness the power of our patients’ data to guide clinical care decisions and make the health care system adaptable to the changing needs of patients.
Finally, I call on VA physician leaders to be innovators, designing and studying new interdisciplinary coordinated models of care, to improve outcomes and then share these models with each other. We physicians need to work together as “One VA” to decrease variability within the system and improve quality and value throughout.
Knee replacement is one of the most commonly performed operations in the United States with over 700,000 procedures performed annually (1). Besides providing anesthesia care in the operating room, anesthesiologists are dedicated to providing the best perioperative pain management in order to improve patients’ function and facilitate rehabilitation after surgery. In the past, pain management was limited to the use of opioids (narcotics). Opioids only attack pain in one way, and just adding more opioids does not usually lead to better pain control.
In 2012, the American Society of Anesthesiologists (ASA) published its guidelines for acute pain management in the perioperative setting (2). This document recommends “multimodal analgesia” which means that two or more classes of pain medications or therapies, working with different mechanisms of action, should be used in the treatment of acute pain.
While opioids are still important pain medications, they should be combined with other classes of medications known to help relieve postoperative pain unless contraindicated. These include:
Non-steroidal anti-inflammatory drugs (NSAIDs): Examples include ibuprofen, diclofenac, ketorolac, celecoxib. NSAIDs act on the prostaglandin system peripherally and work to decrease inflammation.
Acetaminophen: Acetaminophen acts on central prostaglandin synthesis and provides pain relief through multiple mechanisms.
Gabapentinoids: Examples include gabapentin and pregabalin. These medications are membrane stabilizers that essentially decrease nerve firing.
The ASA also strongly recommends the use of regional analgesic techniques as part of the multimodal analgesic protocol when indicated.
Epidural Analgesia
When compared to opioids alone, epidural analgesia produces lower pain scores and shorter time to achieve physical therapy goals (3). However, higher dose of local anesthetic (numbing medicine) may lead to muscle weakness that can limit activity (4). In addition, epidural analgesia can lead to common side effects (urinary retention, dizziness, itchiness) and is not selective for the operative leg, meaning that the non-operative leg may also become numb.
Femoral Nerve Block
A peripheral nerve block of the femoral nerve is specific to the operative leg. When compared to opioids alone, a femoral nerve block provides better pain control and leads to higher patient satisfaction (5). One area of controversy is whether a single-injection nerve block or catheter-based technique is preferred. There is evidence to support the use of continuous nerve block catheters to extend the pain relief and opioid-sparing benefits of nerve blocks in patients having major surgery like knee replacement. When a continuous femoral nerve block catheter is used, the pain relief is comparable to an epidural but without the epidural-related side effects (6). One legitimate concern raised over the use of femoral nerve blocks in knee replacement patients is the resulting quadriceps muscle weakness (7).
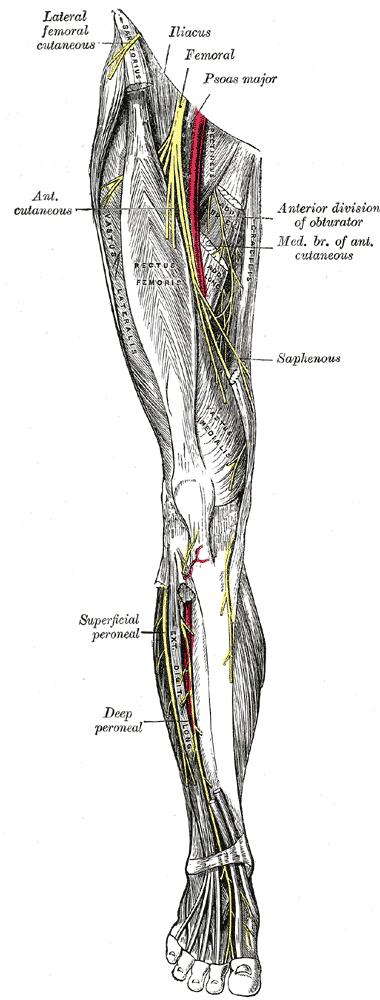
From Gray’s Anatomy
Saphenous Nerve Block (Adductor Canal Block)
The saphenous nerve is the largest sensory branch of the femoral nerve and can be blocked within the adductor canal to provide postoperative pain relief and facilitate rehabilitation (8, 9). In healthy volunteers, quadriceps strength is better preserved when subjects receive an adductor canal block compared to a femoral nerve block (10).
In actual knee replacement patients, quadriceps function decreases regardless of nerve block type after surgery but to a lesser degree with adductor canal blocks (11). Recently there have been reports of quadriceps weakness resulting from adductor canal blocks and catheters that have affected clinical care (12, 13).
Fall Risk
According to a large retrospective study of almost 200,000 cases, the incidence of inpatient falls for patients after TKA is 1.6%, and perioperative use of nerve blocks is not associated with increased risk (14). Patient factors that increase the risk of falls include higher age, male sex, sleep apnea, delirium, anemia requiring blood transfusion, and intraoperative use of general anesthesia (14). The bottom line is that all knee replacement patients are at increased risk for falling due to multiple risk factors, and any clinical pathway should include fall prevention strategies and an emphasis on patient safety.
Other Local Anesthetic Techniques
In addition to a femoral nerve or adductor canal block, a sciatic nerve block is sometimes offered to provide a “complete” block of the leg. There are studies for and against this practice. Arguably, the benefit of a sciatic nerve block does not last beyond the first postoperative day (15). Surgeon-administered local anesthetic around the knee joint (local infiltration analgesia) can be combined with nerve block techniques to provide additional postoperative pain relief for the first few hours after surgery (16, 17).
For more information about anesthetic options for knee replacement, please see my post on My Knee Guide.
American Society of Anesthesiologists Task Force on Acute Pain M: Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 2012, 116(2):248-273.
Mahoney OM, Noble PC, Davidson J, Tullos HS: The effect of continuous epidural analgesia on postoperative pain, rehabilitation, and duration of hospitalization in total knee arthroplasty. Clin Orthop Relat Res 1990(260):30-37.
Raj PP, Knarr DC, Vigdorth E, Denson DD, Pither CE, Hartrick CT, Hopson CN, Edstrom HH: Comparison of continuous epidural infusion of a local anesthetic and administration of systemic narcotics in the management of pain after total knee replacement surgery. Anesth Analg 1987, 66(5):401-406.
Chan EY, Fransen M, Parker DA, Assam PN, Chua N: Femoral nerve blocks for acute postoperative pain after knee replacement surgery. Cochrane Database Syst Rev 2014, 5:CD009941.
Barrington MJ, Olive D, Low K, Scott DA, Brittain J, Choong P: Continuous femoral nerve blockade or epidural analgesia after total knee replacement: a prospective randomized controlled trial. Anesth Analg 2005, 101(6):1824-1829.
Jenstrup MT, Jaeger P, Lund J, Fomsgaard JS, Bache S, Mathiesen O, Larsen TK, Dahl JB: Effects of adductor-canal-blockade on pain and ambulation after total knee arthroplasty: a randomized study. Acta Anaesthesiol Scand 2012, 56(3):357-364.
Hanson NA, Allen CJ, Hostetter LS, Nagy R, Derby RE, Slee AE, Arslan A, Auyong DB: Continuous ultrasound-guided adductor canal block for total knee arthroplasty: a randomized, double-blind trial. Anesth Analg 2014, 118(6):1370-1377.
Kwofie MK, Shastri UD, Gadsden JC, Sinha SK, Abrams JH, Xu D, Salviz EA: The effects of ultrasound-guided adductor canal block versus femoral nerve block on quadriceps strength and fall risk: a blinded, randomized trial of volunteers. Reg Anesth Pain Med 2013, 38(4):321-325.
Jaeger P, Zaric D, Fomsgaard JS, Hilsted KL, Bjerregaard J, Gyrn J, Mathiesen O, Larsen TK, Dahl JB: Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: a randomized, double-blind study. Reg Anesth Pain Med 2013, 38(6):526-532.
Chen J, Lesser JB, Hadzic A, Reiss W, Resta-Flarer F: Adductor canal block can result in motor block of the quadriceps muscle. Reg Anesth Pain Med 2014, 39(2):170-171.
Veal C, Auyong DB, Hanson NA, Allen CJ, Strodtbeck W: Delayed quadriceps weakness after continuous adductor canal block for total knee arthroplasty: a case report. Acta Anaesthesiol Scand 2014, 58(3):362-364.
Abdallah FW, Brull R: Is sciatic nerve block advantageous when combined with femoral nerve block for postoperative analgesia following total knee arthroplasty? A systematic review. Reg Anesth Pain Med 2011, 36(5):493-498.
So, you’ve finished your third year of medical school and have decided that you want to be an anesthesiologist. In our completely biased opinion, you are making the right choice and, at the end of your residency training, you will be in a unique position to enhance the experience and improve the outcomes of patients undergoing surgery and invasive procedures. However, securing a coveted slot in an anesthesiology residency in the United States has never been more competitive. In the many years that we have spent as faculty in academic anesthesiology departments, we have learned a few things about the application process. Our views are our own and do not reflect the official views of any anesthesiology residency program with which we have been affiliated. The following are some (hopefully helpful) answers to common questions that we have been asked over the years.
How High Do My USMLE Score and GPA Have to Be?
Competitive scores are essential. We can’t quote you a number because they vary year to year and program to program, but the trend is only increasing. All medical students, regardless of school, applying in anesthesiology must do well on the USMLE. Think about it — this is the only equalizing factor between schools that teach differently or have different reputations. Having a great score doesn’t guarantee you admission, but if your scores are not competitive, you will have an uphill battle to get a residency slot at a top program. The value of the standardized test score in learning is often debated in academia; however, no one will argue against the conclusion that previous success on standardized tests usually predicts future success on standardized tests. Residency training is demanding. Programs want their residents 100 percent committed and not worrying too much about how they will perform on their annual in-training exams and eventual certification exam.
Do I Need to Have Research Experience?
No program will ever discourage applicants with research experience from applying; we would say that it is not required but is recommended. Don’t do it for the sake of doing it, but definitely do it if you can find a project that you are passionate about. While research in anesthesiology or pain makes sense (shows academic interest in the chosen field), it can really be in any area. It is more impressive to be involved in a project (big or small), see it through, and maybe even present at a meeting or publish in a journal, than to just say you did “research.” If you do list research on your application or curriculum, make sure you can talk about the project, your specific role, and what you learned from it; you will be asked. If you are not interested in research, then consider focusing on another aspect of extracurricular life such as community service.
What Should Be on My List of Extracurricular Activities?
If there is something about you that is really different, it’s helpful to mention it. Again, the application process isn’t perfect, but the file you submit is all the information program coordinators and directors have. If you have done something special — climbed Mt. Everest, set up HIV clinics in Africa, won Olympic medals, had a previous career — or do something noteworthy, such as volunteer extensively in your community, play an instrument, or dance professionally, mention those things. Yes, we have actually seen these applicants (and interviewed them of course)! Selection committee members often apply the “3 a.m. call rule” when reviewing an applicant. This is: Would you like to be on call in the middle of the night with this person? Applicants viewed as hardworking, clinically competent, and interesting to talk to should result in a solid “yes.” If you just like to run in your free time, mentioning that probably doesn’t make a huge difference in the application.
Do I Need to Do an Anesthesiology Rotation?
You should do an anesthesiology rotation at your local institution at the very least. Programs want to know if you understand what you’re getting yourself into. And it does make a difference how well you did on the rotation. Many students approach their anesthesiology rotation as the “intubation and IV insertion” rotation. Most anesthesiologists like us are passionate about their specialty, and the specialty itself in rapidly evolving (familiarize yourself with the Perioperative Surgical Home model). Trust us — we can tell when a student is genuinely interested in anesthesiology, or not. In our experience, medical students who stand out pay attention to what is going on in the perioperative period, anticipate events, know how to be helpful, get involved with the entire patient care episode (starting with the preoperative evaluation, through giving report to the nurse in the recovery room, and even including postoperative follow-up). It is never impressive to see a medical student standing around looking bored. There is always something to do — for example, when a patient arrives in the OR, you can start applying monitors without prompting, or help with positioning. Residents and staff anesthesiologists recognize these things and reward you by getting you more involved with patient care, including procedures.
Who Should Write My Letters of Recommendation?
The dean’s letter is the big one and counts the most. The form of the dean’s letter is usually standardized, so residency program directors have to weed through all the verbiage to get the information they want. It helps when the dean’s letter includes the student’s rank and any special merits (e.g., AOA). Additional letters should be written by faculty members who really know you and can provide helpful content — research mentor, career advisor, staff physician with whom you have worked closely. It doesn’t add strength to an application to have a lot of generic letters (quality over quantity); three strong letters are better than two strong plus three average letters, since the strong letters may get lost in the sea of information in the applicant’s file.
What Else Can I Do to Improve My Chances?
Unfortunately there are no guarantees. The “gatekeeper” is the initial electronic application. With anesthesiology departments receiving hundreds of applications each year, most will sound exactly the same. “I love pharmacology and physiology” (while possibly true for some) only takes you so far. Something unique about the applicant has to come through the pages. Excellent grades and USMLE scores, strong dean’s letter and other recommendations, personal experiences, prior careers, other degrees, thought-provoking research, a list of activities, and a unique personal statement — anything that sets you apart from the pack can make a difference!
I wear a lot of hats in my job. Though I’m a physician who specializes in the practice of anesthesiology, I don’t spend all day every day at the head of an operating room table.
Many days I spend in an administrative leadership role or conducting research studies. These functions support the best interests of my patients as well as the science and practice of anesthesiology. On my “clinical” days that I spend in hands-on patient care, I provide anesthesia for patients who undergo surgery and other invasive procedures. I also treat acute pain as a consultant. Some of my colleagues in anesthesiology specialize in chronic pain or critical care medicine.
As a medical student, I had a hard time at first understanding what the physician anesthesiologist does. I saw monitors, complicated equipment, and technical procedures that involved a lot of needles. Thankfully, I worked with resident and attending anesthesiologists who inspired me to pursue this specialty.
Anesthesiology is a unique field within medicine. It is at the same time incredibly cerebral and extremely physical. For example, the physician anesthesiologist must be ready to diagnose heart or lung problems that may complicate the patient’s surgery, and decide which medications are appropriate.
Before administering a medication, it’s not enough just to understand the complex pharmacologic effects of the drug and determine the right dose. The anesthesiologist also has to know how to dilute and prepare the drug, the appropriate route for the medication, which other medications are and are not compatible, and how to program the infusion device. In addition, an anesthesiologist has to be technically skilled at finding veins—sometimes in the hand or arm, sometimes leading centrally to the heart—in order to give the medication in the first place.
I am always aware of the trust that patients and their families give me, a total stranger, and I work hard to earn that trust throughout the perioperative period. The job of the physician anesthesiologist is deeply personal. In the operating room, I care for the most vulnerable of patients—those who, while under anesthesia, cannot care for themselves.
– I constantly listen to the sounds of their hearts. – I breathe for them when they are unable. – I keep them warm in the cold operating room. – I provide the fluids that their bodies need. – I pad their arms and legs and other pressure points. – I watch the operation step by step, anticipating and responding. – I learn from their bodies’ response to anesthesia to give the right amount. – I prevent and relieve their pain. – I protect them from dangers of which they are unaware.
I have heard people, my colleagues included, compare physician anesthesiologists to pilots. No one claps when the plane lands, just as no one expects any less than a perfect uncomplicated anesthetic every time. We physician anesthesiologists draw great personal satisfaction from doing what we do, and from providing a unique type of personalized medicine. Our patients and their families depend on us to be at our best, always.
The concept of preoperative preparation for patients scheduled for surgery requiring anesthesia is not a new one. In fact, the idea goes back to Dr. Albert Lee’s description in 1949 (1, 2). Dr. Lee had observed in his day that patients commonly presented for surgery in various states of poor health; it seemed to make more sense to see these patients before surgery to identify areas of concern early and optimize patients’ conditions they went under the knife.
The model of a stand-alone preoperative evaluation clinic, often run by anesthesiology staff, with a “one stop shop” model for patients’ interviews and examinations, testing, education, and referrals really did not take off until the 1990s (3). This patient-centered care model was intended to improve efficiency by decreasing the run-around that many patients encountered, but it also saved money for the institution by reducing the ordering of unnecessary tests (4) and decreasing day-of-surgery cancellations (4, 5).
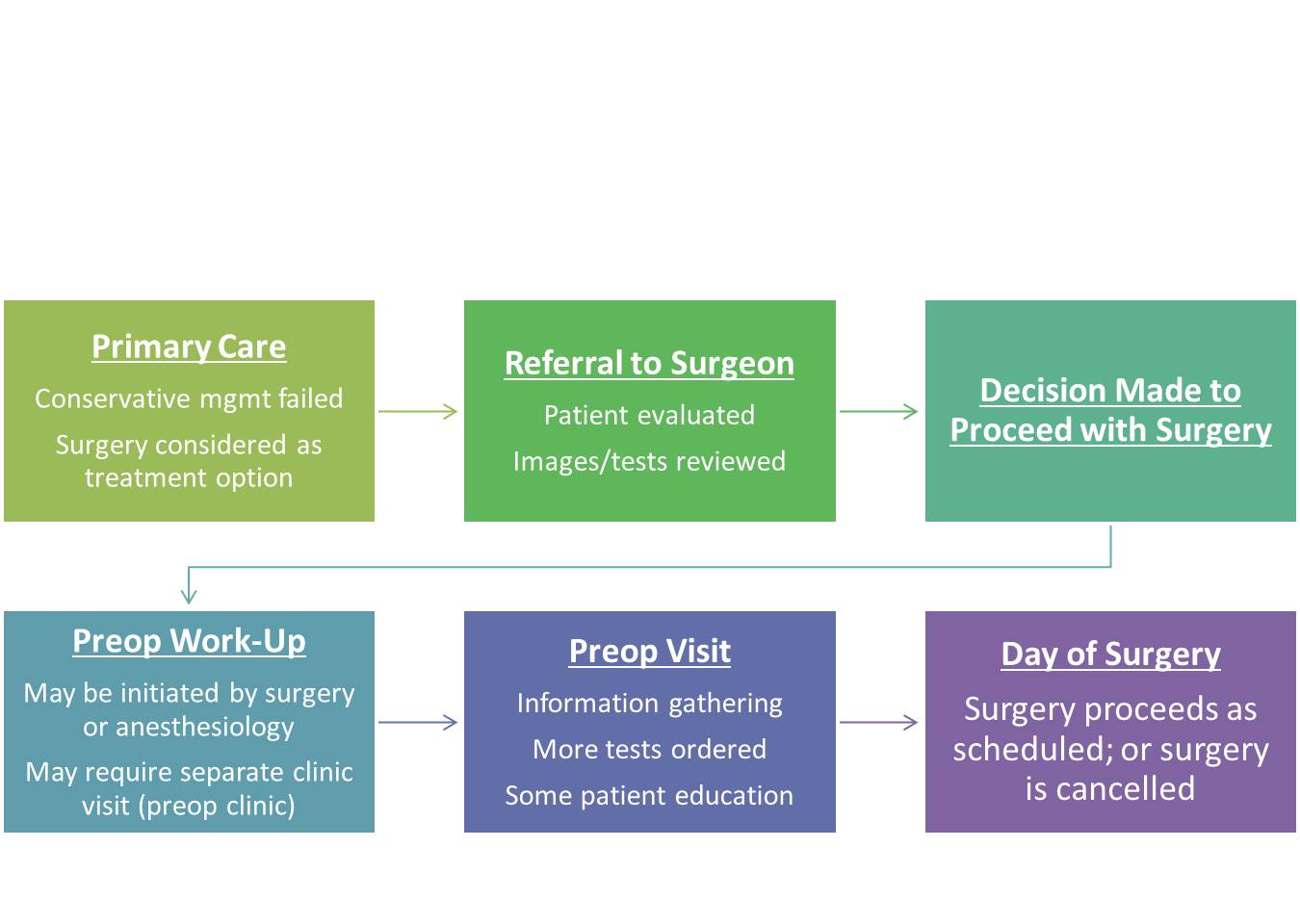
Current State
In the present state (assuming an ACO or HMO model), patients are referred to the surgeon by the primary care physician for evaluation of a problem that may be amenable to surgical correction. If the surgeon deems the patient a surgical candidate, the patient may receive a scheduled date for surgery and then may be referred to the anesthesiology preoperative evaluation clinic (“preop clinic”) for further work-up. During this encounter, the provider in the preop clinic may request a variety of tests based on the planned surgery and the patient’s comorbid conditions in order to make appropriate recommendations regarding perioperative management to minimize risks. The American Society of Anesthesiologists (ASA) has published a recent (2012) practice advisory for preanesthesia evaluation to guide this process.
Unfortunately, after nearly 2 decades of employing this model, day of surgery cancellations still occur at various rates around the world. Some of the reasons are related to factors that preop clinics were meant to avoid: inadequate preoperative work-up or change in medical condition (6). Other reasons are patient-driven: patients’ not showing up (7) or patients’ changing their minds about having surgery (8). Although not all of these issues are easily solved, it does make me wonder–perhaps it is time for us to rethink the process of preparing patients for surgery.
In our current state, a patient may hypothetically be scheduled for surgery in 8 weeks, a date agreed upon by the patient and surgeon based on available dates. Even if a preop clinic visit takes place the same day as the surgery clinic visit, this only allows 2 months to optimize a patient’s chronic medical conditions (e.g., hypertension, diabetes, coronary artery disease) that took years to develop. Imagine if the timeline was even shorter, like 3 weeks. Add to this time pressure the tremendous physiologic stress that surgery and the subsequent rehabilitation put on the body, and it is not difficult to see why patients can still be cancelled on the day of surgery when they present with abnormal vital signs or test results, making the risks seem too high. We would not expect ourselves to run a marathon without adequate training and preparation on short notice–why would we do this to our patients having elective surgery?
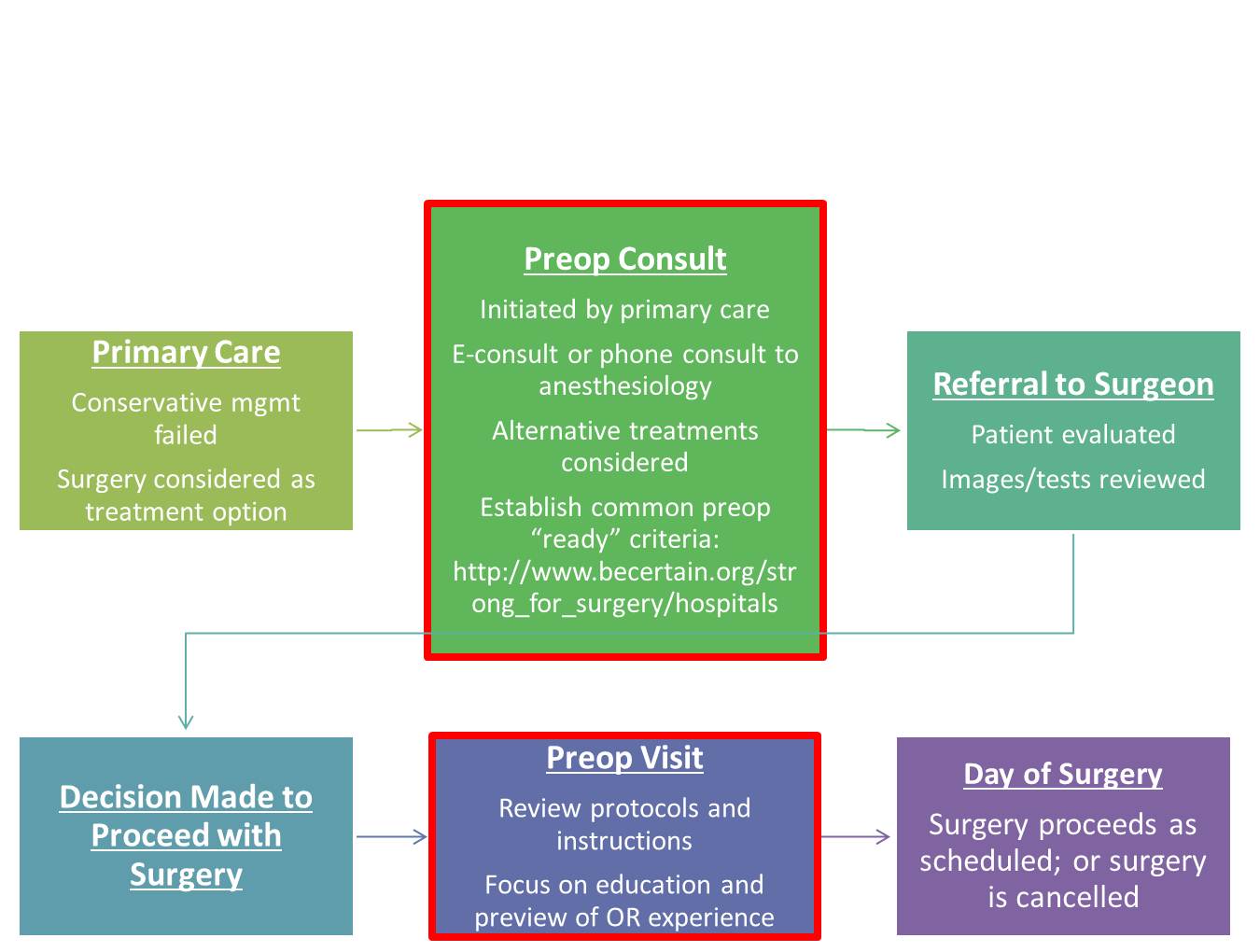
Future State
How can we improve preoperative preparation? I think it still starts with the primary care physician. With advances in technology such as telemedicine and e-consults (or low-tech phone calls), we have ways to create a direct interface between primary care physicians and anesthesiologists to discuss advanced preparation of patients who may undergo elective surgical procedures.
This coordinated care model is consistent with ASA’s Perioperative Surgical Home. Early consultation may involve assessment of a patient’s risks and benefits from the procedure, consideration of alternative treatments, and development of a plan to optimize the patient’s comorbid conditions, medication management, and nutrition. Strong for Surgery is a program that provides patients and clinicians useful checklists based on best-available evidence to guide early preoperative preparation related to smoking cessation, nutrition, glycemic control, and medication management. For elective surgery, the decision when to refer the patient to a surgeon can be made jointly by the primary care physician and anesthesiologist. Prior to surgery, the preop clinic visit should still take place, but the focus no longer needs to be on information-gathering and ordering a battery of tests; rather, the goals should be to review pertinent instructions, preview the perioperative experience for patients, and address any logistical or scheduling issues raised by patients to prevent their not showing up or changing their minds at the last minute. Let’s get started.
Chronic pain can be palliated, but “acute” pain (new onset, often with an identifiable cause) must be stamped out. This requires a systems-based approach led by physicians dedicated to understanding acute pain pathophysiology and investigating new ways to treat it. The solution is definitely not giving more and more opioids.
As our understanding of pain mechanisms has evolved, select physicians have developed a special focus on pain in the acute injury/illness and perioperative settings that has led to the rapid advancement of systemic and site-specific interventions to effectively manage this type of pain. Acute pain medicine involves the routine use of multiple modalities concurrently (i.e., multimodal analgesia) in the in-hospital setting to reduce the intensity of acute pain and minimize the development of debilitating persistent pain, a problem that can result from even common surgical procedures or trauma. Unfortunately, the need for specialists in acute pain medicine is increasing.
In December of 2013, I submitted a 161 page letter to the Accreditation Council for Graduate Medical Education (ACGME) requesting that regional anesthesiology and acute pain medicine be considered for fellowship accreditation with the help of my fellowship director colleagues. The Board of Directors of the ACGME informed me this past fall (2014) that they have approved our fellowship to be the next accredited subspecialty within anesthesiology.
Wait – don’t we already have a fellowship program in pain medicine? Yes we do, and this one year post-residency program does include the “Acute Pain Inpatient Experience.” However, this requirement may be satisfied by documented involvement with a minimum of only 50 new patients and is not the primary emphasis of fellowship training in the specialty. Pain medicine is a board-certified subspecialty of anesthesiology, physical medicine and rehabilitation, and psychiatry and neurology; graduates from any of these residency programs can apply to the one year program. In a recent survey study of practicing pain physicians in the United States with added qualification in pain management according to the American Board of Medical Specialties (ABMS), the great majority (83.7%) of respondents defined their practices as following “chronic pain patients longitudinally” (1).
There is clearly room and a need for a subspecialty training program in acute pain medicine that can focus on improving the in-hospital pain experience. Such a program should advance, in a positive and value-added fashion, the present continuum of training in pain medicine.
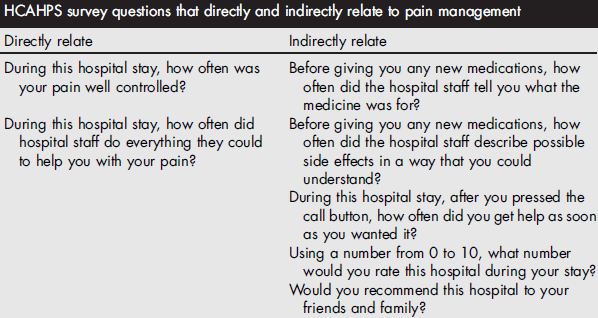
The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey is administered to a random sample of patients who have received inpatient care and receive government insurance through Center for Medicare and Medicaid Services (CMS). The survey consists of 32 questions and is intended to assess the “patient experience of care” domain in the value-based purchasing program. A hospital’s survey scores are publicly disclosed and make up 30% of the formula used to determine how much of its diagnosis-related group payment withholding will be paid by CMS at the end of each year. Of the 32 questions, 7 directly or indirectly relate to in-hospital pain management.
Why should acute pain medicine be a subspecialty of anesthesiology? Anesthesiology is a hospital-based medical specialty, and anesthesiologists are physicians who focus on the prevention and treatment of pain for their patients who undergo surgery, suffer trauma, or present for childbirth on a daily basis. For more details on the role of the anesthesiologist, please see “Physicians specializing in the patient experience.” Further, history supports the evolution of acute pain medicine through anesthesiology. The concept of an anesthesiology-led acute pain management service was described first in 1988 (2), but arguably the techniques employed in modern acute pain medicine and regional anesthesiology date back to Gaston Labat’s publication of Regional Anesthesia: its Technic and Clinical Application in 1922, with advancement and refinement of this subspecialty in the 1960s and 1970s (3-7).
By the time they complete the core residency in anesthesiology today, not all trainees have gained sufficient clinical experience to provide optimal care for the complete spectrum of issues experienced by patients suffering from acutely painful conditions, including the ability to reliably provide advanced interventional techniques proven to be effective in managing pain in the acute setting (8-12). We need physician leaders who can run acute pain medicine teams and design systems to provide individualized, comprehensive, and timely pain management for both medical and surgical patients in the hospital, expeditiously managing requests for assistance when pain intensity levels exceed those set forth in quality standards, or to prevent pain intensity from reaching such levels. The mission statement for the Acute Pain Medicine Special Interest Group within the American Academy of Pain Medicine provides additional justification.
In a survey of fellowship graduates and academic chairs published in 2005, 61 of 132 of academic chairs responded (46%), noting that future staffing models for their department will likely include an average of 2 additional faculty trained in regional anesthesiology and acute pain medicine (13).
Currently, there are over 60 institutions in the United States and Canada that list themselves as having non-accredited fellowship training programs focused on regional anesthesiology and acute pain medicine on the ASRA website. Since 2002, the group of regional anesthesiology and acute pain medicine fellowship directors has been meeting twice yearly at the ASRA Spring Annual Meeting and ASA Annual Meeting which takes place in the fall. Despite not being an ACGME-accredited fellowship, this group, recognizing the lack of formalized training guidelines, voluntarily began to develop such guidelines as the foundation for subspecialty fellowship training in existing and future programs. These guidelines were originally published in Regional Anesthesia and Pain Medicine in 2005 (14), then were subsequently reviewed, revised, and published as the 2nd edition in 2011 (15), and have been recently updated again (16).
As with other subspecialties, acute pain medicine has emerged due to the need for trained specialists—in this case, those who understand the complicated, multi-faceted disease processes of acute pain, and its potential continuity with chronic pain, and can apply appropriate medical and interventional treatment in a timely fashion. The fellowship-trained regional anesthesiologist and acute pain medicine specialist must be capable of collaborating with other healthcare providers in anesthesiology, surgery, medicine, nursing, pharmacy, physical therapy, and more to establish multidisciplinary programs that add value and improve patient care in the hospital setting and beyond.
REFERENCES
Breuer B, Pappagallo M, Tai JY, Portenoy RK: U.S. board-certified pain physician practices: uniformity and census data of their locations. J Pain 2007; 8: 244-50
Ready LB, Oden R, Chadwick HS, Benedetti C, Rooke GA, Caplan R, Wild LM: Development of an anesthesiology-based postoperative pain management service. Anesthesiology 1988; 68: 100-6
Winnie AP, Ramamurthy S, Durrani Z: The inguinal paravascular technic of lumbar plexus anesthesia: the “3-in-1 block”. Anesth Analg 1973; 52: 989-96
Winnie AP, Collins VJ: The Subclavian Perivascular Technique of Brachial Plexus Anesthesia. Anesthesiology 1964; 25: 353-63
Raj PP, Parks RI, Watson TD, Jenkins MT: A new single-position supine approach to sciatic-femoral nerve block. Anesth Analg 1975; 54: 489-93
Raj PP, Rosenblatt R, Miller J, Katz RL, Carden E: Dynamics of local-anesthetic compounds in regional anesthesia. Anesth Analg 1977; 56: 110-7
Buvanendran A, Kroin JS: Multimodal analgesia for controlling acute postoperative pain. Curr Opin Anaesthesiol 2009; 22: 588-93
Hebl JR, Dilger JA, Byer DE, Kopp SL, Stevens SR, Pagnano MW, Hanssen AD, Horlocker TT: A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. Reg Anesth Pain Med 2008; 33: 510-7
Jin F, Chung F: Multimodal analgesia for postoperative pain control. J Clin Anesth 2001; 13: 524-39
Kehlet H, Dahl JB: The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg 1993; 77: 1048-56
Young A, Buvanendran A: Recent advances in multimodal analgesia. Anesthesiol Clin 2012; 30: 91-100
Neal JM, Kopacz DJ, Liguori GA, Beckman JD, Hargett MJ: The training and careers of regional anesthesia fellows–1983-2002. Reg Anesth Pain Med 2005; 30: 226-32
This year’s American Society of Regional Anesthesia and Pain Medicine’s 13th Annual Fall Pain Medicine meeting happens to be in my “neck of the woods”—one of the greatest cities in the world—San Francisco, California. Here are a few things you may or may not have known about San Francisco.
San Francisco is the biggest little city. At just under 47 square miles and with more than 200,000 inhabitants, San Francisco is second only to New York City in terms of population density. Despite its relatively small size, “the City” (as we suburbanites refer to it) consists of many small neighborhoods, each with its own charm and character: Union Square, the Financial District, Pacific Heights, the Marina, Haight-Ashbury, Chinatown, Little Italy, Nob Hill, Russian Hill, SoMa (South of Market), the Fillmore, Japantown, Mission District, Noe Valley, Twin Peaks, Castro, Sunset, Tenderloin, and others. For this reason, San Francisco may arguably be the only option for die-hard New Yorkers who wish to relocate away from snow.
Chinatown
Even though it doesn’t snow, San Francisco weather is incredibly unpredictable, even when going from one side of the city to the other. “The coldest winter I ever spent was a summer in San Francisco,”a quote often mistakenly attributed to Mark Twain (no one really knows who actually said it), is nevertheless often true. Here in the San Francisco Bay Area, our local meteorologists provide daily forecasts for each of the region’s microclimates. The western side of the City along California’s coast is regularly plagued with fog while the eastern side of the City tends to be sunny most days of the year. It’s always a good idea to check the microclimate forecast before heading over to see the Golden Gate Bridge just in case it happens to be shrouded in fog. Also, average July temperatures in the City range in the 50s-60s Fahrenheit (no different than average November temperatures), so summer tourists often contribute to the local economy by buying “SF” logo sweatshirts for their walk across the City’s most famous bridge.
Ferry Building
San Francisco is very family-friendly. If you’re debating whether or not to make a family trip out of the Fall Pain Meeting, my advice is to do it. Right around the conference hotel, the Hyatt Regency San Francisco, there are a number of attractions and events worth checking out. Every Saturday there is a huge farmers market at the Ferry Building across the street from the hotel. As you probably figured out, from the Ferry Building you can also take a ferry ride to a number of other destinations in the Bay Area (I recommend Sausalito, a short trip that takes you past Alcatraz). For kids, there are 3 parks within walking distance, the San Francisco Railway Museum, Exploratorium, and the cable car turnabout at Powell and Market Street; trips to Fisherman’s Wharf or the aquarium are a short taxi or cable car ride away. In addition, runners will love running up and down the Embarcadero which gives you a view of the Bay Bridge and takes you past the City’s many piers; shoppers will be in heaven; and foodies have an impossible decision to make when choosing the location for every meal (try Slanted Door at the Ferry Building at least once).
Enough about San Francisco—you’ll have to see it for yourself. To register for the Fall Pain Medicine meeting, visit http://www.asrameetings.com/. For an overview of scheduled events in the words of meeting Chair, Dr. David Provenzano, see the August 2014 issue of ASRA News. This issue also includes fantastic original content covering the topics of digital subtraction angiography, pain outcomes, ASRA’s first entry into the app market, and much more!
Among Medicare beneficiaries in the United States, the number of primary total knee arthroplasty (TKA) procedures from 1991 to 2010 increased by 161.5% (1). Postoperative pain remains one of patients’ top concerns when undergoing elective surgery (2) and can limit patients’ functional ability in the early postoperative period (3). Providing effective perioperative pain control has potential longer-term implications since early rehabilitation may lead to improvements in functional outcomes later on (4). With the ability to select specific targets for local anesthetic injection and infusion, regional anesthesia techniques, neuraxial and peripheral, are commonly included in the perioperative analgesic protocol for joint arthroplasty patients (5-11). While the data supporting the analgesic efficacy of regional anesthesia techniques in this setting are strongly positive, studies attempting to attribute functional outcome benefits to regional anesthesia demonstrate mixed results.
The main challenge in assessing functional outcomes following joint replacement is the selection of outcomes; these can be divided into performance-based outcomes and self-reported outcomes (12, 13). Performance-based outcomes are measurable and arguably more objective, although often subject to effort. Examples of these outcomes and their units of measure include joint range of motion in degrees (e.g., flexion, extension, rotation); timed walking tests in meters (e.g., 6 minute walking test [6MWT], 2 minute walking test [2MWT]); muscle strength in units of force using a dynamometer (e.g., maximum voluntary isometric contraction [MVIC]); and timed up-and-go (TUG) in minutes (12, 13). Self-reported outcomes are typically survey-based; examples include the Western Ontario McMaster Universities Osteoarthritis Index (WOMAC), Knee Society Score, and Lower Extremity Functional Scale (12, 13). Since patient perception of successful rehabilitation is an important factor, self-reported outcomes should be reported with performance-based outcomes (12). Another important challenge when measuring and comparing functional outcomes is that clinical pathways for joint arthroplasty that integrate pain management (including regional analgesia), physical therapy, nursing, and surgical care are often specific to individual institutions, and institutions may vary with respect to rehabilitation goals and the timeline to achieve them.
Epidural Analgesia
Epidural analgesia has been used for perioperative pain management in joint replacement patients since at least the 1980s (14, 15). In 1987, Raj and colleagues compared postoperative systemic opioid analgesia to continuous epidural analgesia (bupivacaine 0.25% at 6-15 ml/hr) for TKA patients in a prospective non-randomized study (14). Although pain scores were lower in the epidural group, not surprisingly a high proportion of these patients experienced complete motor block of the lower extremities; although the authors mention “rigorous passive exercises,” specific rehabilitation outcomes were not reported (14). Later studies have reported functional benefits associated with continuous epidural analgesia, such as shorter time to achieve ambulation distance and range of motion goals, when compared to parenteral opioids alone (16). At institutions where continuous epidural analgesia is currently employed as part of a multimodal analgesic protocol, very low doses of local anesthetic (e.g., 0.06% bupivacaine) in combination with opioid are used in order to minimize motor block (17).
Peripheral Nerve Blocks
The innervation of the knee is complex and involves contributions from both the lumbar and sacral plexuses. While epidural analgesia is effective, it is also associated with clinically-significant side effects (e.g., nausea/vomiting and motor block of the non-operative limb) (5, 18) and the potential for neuraxial hematoma in patients on pharmacologic thromboprophylaxis (19). Thus, peripheral nerve block options, either single-injection or continuous infusions, have been explored for postoperative pain management.
Two early studies by Capdevila (6) and Singelyn (20) have shown continuous femoral nerve block (FNB) to provide comparable analgesia and physical therapy outcome achievement with fewer side effects when compared to epidural analgesia. Both of these studies also demonstrated shorter hospital length of stay for the regional anesthesia groups compared to an opioid-only group (6, 20), but hospitalization duration for these studies was, on average, greater than what has been reported in other studies (21). Triple-masked, placebo-controlled randomized clinical trials have shown that CPNB can shorten the time to achieve discharge criteria, including 100 m ambulation distance, for TKA (10, 22) and total hip arthroplasty (THA) (9) patients, but actual hospital duration was similar in these studies.
One of the interesting findings from the Singelyn study was that regional anesthesia patients maintained a knee flexion advantage over the opioid-only group at 6 week follow-up (20); although this advantage did not remain at 3 months, this finding supported the potential for long-term functional improvement resulting from effective pain management and early rehabilitation in the immediate perioperative period (4). In a randomized comparison of continuous FNB to local infiltration analgesia (LIA) for TKA, the FNB group spent more time out of bed walking; at 6 weeks, the FNB group showed more improvement in performance-based (6MWT) and self-reported functional outcome assessments (23). In contrast, the one year follow-up studies of randomized clinical trial subjects (9, 10, 22) using self-reported outcome measures for functional status (WOMAC) did not show long-term improvement associated with regional anesthesia techniques (24-27).
The rehabilitation outcome measured in the immediate postoperative period that correlates best with long-term functional improvement is not yet established. Ambulation distance is often measured by physical therapists and included in discharge criteria (9, 10, 22). For institutions that emphasize ambulation in their clinical pathway for lower extremity joint arthroplasty, a major concern raised with regard to FNBs is the potential association with increased fall risk (28, 29) although a recent large database study disputes this finding. In-hospital falls can lead to prolonged hospital stays with higher costs and are associated with more frequent postoperative complications, including serious organ system dysfunction and death (30). With currently-available local anesthetic solutions and typical doses, perineural infusion does produce clinically-significant quadriceps weakness when administered near the femoral nerve or lumbar plexus (31, 32). Since the local anesthetics themselves cannot select sensory over motor nerves( 33), anesthesiologists have started exploring alternate nerve block locations to minimize the risk of motor block and maximize patient rehabilitation.
From Workman JJ, et al. Presented at 2013 ASRA Spring Annual Meeting
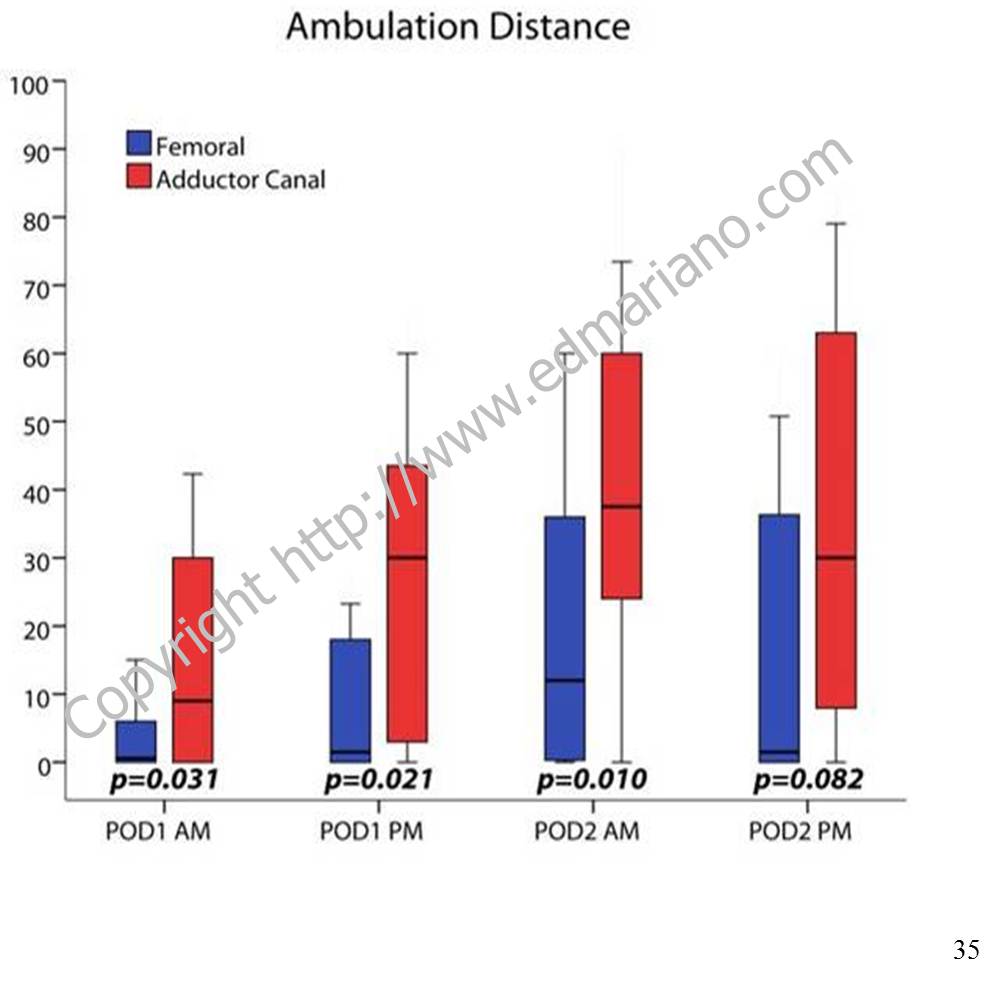
For TKA, a more distal nerve block location in the adductor canal can provide effective analgesia postoperatively (34) and has been shown to better preserve quadriceps strength compared to a FNB in both volunteers (35) and clinical patients (11). Regional analgesic techniques are only one part of the overall pain management plan. While they are often included in multimodal analgesic protocols along with non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and low-dose opioids (36), there is a growing body of evidence to support the adductor canal block as the regional analgesic technique of choice for promoting postoperative ambulation within a clinical pathway (37, 38).
For patient information with answers to frequently-asked questions about regional anesthesia, please see “Regional Anesthesia FAQs.”
References
Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991-2010. JAMA. Sep 26 2012;308(12):1227-1236.
Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg. Sep 1999;89(3):652-658.
Holm B, Kristensen MT, Myhrmann L, et al. The role of pain for early rehabilitation in fast track total knee arthroplasty. Disability and rehabilitation. 2010;32(4):300-306.
Munin MC, Rudy TE, Glynn NW, Crossett LS, Rubash HE. Early inpatient rehabilitation after elective hip and knee arthroplasty. JAMA. Mar 18 1998;279(11):847-852.
Barrington MJ, Olive D, Low K, Scott DA, Brittain J, Choong P. Continuous femoral nerve blockade or epidural analgesia after total knee replacement: a prospective randomized controlled trial. Anesth Analg. Dec 2005;101(6):1824-1829.
Capdevila X, Barthelet Y, Biboulet P, Ryckwaert Y, Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology. Jul 1999;91(1):8-15.
Chelly JE, Greger J, Gebhard R, et al. Continuous femoral blocks improve recovery and outcome of patients undergoing total knee arthroplasty. J Arthroplasty. Jun 2001;16(4):436-445.
Hebl JR, Dilger JA, Byer DE, et al. A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. Reg Anesth Pain Med. Nov-Dec 2008;33(6):510-517.
Ilfeld BM, Ball ST, Gearen PF, et al. Ambulatory continuous posterior lumbar plexus nerve blocks after hip arthroplasty: a dual-center, randomized, triple-masked, placebo-controlled trial. Anesthesiology. Sep 2008;109(3):491-501.
Ilfeld BM, Le LT, Meyer RS, et al. Ambulatory continuous femoral nerve blocks decrease time to discharge readiness after tricompartment total knee arthroplasty: a randomized, triple-masked, placebo-controlled study. Anesthesiology. Apr 2008;108(4):703-713.
Jaeger P, Zaric D, Fomsgaard JS, et al. Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: a randomized, double-blind study. Reg Anesth Pain Med. Nov-Dec 2013;38(6):526-532.
Choi S, Trang A, McCartney CJ. Reporting functional outcome after knee arthroplasty and regional anesthesia: a methodological primer. Reg Anesth Pain Med. Jul-Aug 2013;38(4):340-349.
Bernucci F, Carli F. Functional outcome after major orthopedic surgery: the role of regional anesthesia redefined. Curr Opin Anaesthesiol. Oct 2012;25(5):621-628.
Raj PP, Knarr DC, Vigdorth E, et al. Comparison of continuous epidural infusion of a local anesthetic and administration of systemic narcotics in the management of pain after total knee replacement surgery. Anesth Analg. May 1987;66(5):401-406.
Pettine KA, Wedel DJ, Cabanela ME, Weeks JL. The use of epidural bupivacaine following total knee arthroplasty. Orthopaedic review. Aug 1989;18(8):894-901.
Mahoney OM, Noble PC, Davidson J, Tullos HS. The effect of continuous epidural analgesia on postoperative pain, rehabilitation, and duration of hospitalization in total knee arthroplasty. Clin Orthop Relat Res. Nov 1990(260):30-37.
YaDeau JT, Cahill JB, Zawadsky MW, et al. The effects of femoral nerve blockade in conjunction with epidural analgesia after total knee arthroplasty. Anesth Analg. Sep 2005;101(3):891-895, table of contents.
Zaric D, Boysen K, Christiansen C, Christiansen J, Stephensen S, Christensen B. A comparison of epidural analgesia with combined continuous femoral-sciatic nerve blocks after total knee replacement. Anesth Analg. Apr 2006;102(4):1240-1246.
Horlocker TT, Wedel DJ, Rowlingson JC, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Reg Anesth Pain Med. Jan-Feb 2010;35(1):64-101.
Singelyn FJ, Deyaert M, Joris D, Pendeville E, Gouverneur JM. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous three-in-one block on postoperative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg. Jul 1998;87(1):88-92.
Salinas FV, Liu SS, Mulroy MF. The effect of single-injection femoral nerve block versus continuous femoral nerve block after total knee arthroplasty on hospital length of stay and long-term functional recovery within an established clinical pathway. Anesth Analg. Apr 2006;102(4):1234-1239.
Ilfeld BM, Mariano ER, Girard PJ, et al. A multicenter, randomized, triple-masked, placebo-controlled trial of the effect of ambulatory continuous femoral nerve blocks on discharge-readiness following total knee arthroplasty in patients on general orthopaedic wards. Pain. Sep 2010;150(3):477-484.
Carli F, Clemente A, Asenjo JF, et al. Analgesia and functional outcome after total knee arthroplasty: periarticular infiltration vs continuous femoral nerve block. Br J Anaesth. Aug 2010;105(2):185-195.
Ilfeld BM, Shuster JJ, Theriaque DW, et al. Long-term pain, stiffness, and functional disability after total knee arthroplasty with and without an extended ambulatory continuous femoral nerve block: a prospective, 1-year follow-up of a multicenter, randomized, triple-masked, placebo-controlled trial. Reg Anesth Pain Med. Mar-Apr 2011;36(2):116-120.
Morin AM, Kratz CD, Eberhart LH, et al. Postoperative analgesia and functional recovery after total-knee replacement: comparison of a continuous posterior lumbar plexus (psoas compartment) block, a continuous femoral nerve block, and the combination of a continuous femoral and sciatic nerve block. Reg Anesth Pain Med. Sep-Oct 2005;30(5):434-445.
Ilfeld BM, Ball ST, Gearen PF, et al. Health-related quality of life after hip arthroplasty with and without an extended-duration continuous posterior lumbar plexus nerve block: a prospective, 1-year follow-up of a randomized, triple-masked, placebo-controlled study. Anesth Analg. Aug 2009;109(2):586-591.
Ilfeld BM, Meyer RS, Le LT, et al. Health-related quality of life after tricompartment knee arthroplasty with and without an extended-duration continuous femoral nerve block: a prospective, 1-year follow-up of a randomized, triple-masked, placebo-controlled study. Anesth Analg. Apr 2009;108(4):1320-1325.
Feibel RJ, Dervin GF, Kim PR, Beaule PE. Major complications associated with femoral nerve catheters for knee arthroplasty: a word of caution. J Arthroplasty. Sep 2009;24(6 Suppl):132-137.
Ilfeld BM, Duke KB, Donohue MC. The association between lower extremity continuous peripheral nerve blocks and patient falls after knee and hip arthroplasty. Anesth Analg. Dec 2010;111(6):1552-1554.
Memtsoudis SG, Dy CJ, Ma Y, Chiu YL, Della Valle AG, Mazumdar M. In-hospital patient falls after total joint arthroplasty: incidence, demographics, and risk factors in the United States. J Arthroplasty. Jun 2012;27(6):823-828 e821.
Charous MT, Madison SJ, Suresh PJ, et al. Continuous femoral nerve blocks: varying local anesthetic delivery method (bolus versus basal) to minimize quadriceps motor block while maintaining sensory block. Anesthesiology. Oct 2011;115(4):774-781.
Ilfeld BM, Moeller LK, Mariano ER, et al. Continuous peripheral nerve blocks: is local anesthetic dose the only factor, or do concentration and volume influence infusion effects as well? Anesthesiology. Feb 2010;112(2):347-354.
Ilfeld BM, Yaksh TL. The end of postoperative pain–a fast-approaching possibility? And, if so, will we be ready? Reg Anesth Pain Med. Mar-Apr 2009;34(2):85-87.
Lund J, Jenstrup MT, Jaeger P, Sorensen AM, Dahl JB. Continuous adductor-canal-blockade for adjuvant post-operative analgesia after major knee surgery: preliminary results. Acta Anaesthesiol Scand. Jan 2011;55(1):14-19.
Jaeger P, Nielsen ZJ, Henningsen MH, Hilsted KL, Mathiesen O, Dahl JB. Adductor Canal Block versus Femoral Nerve Block and Quadriceps Strength: A Randomized, Double-blind, Placebo-controlled, Crossover Study in Healthy Volunteers. Anesthesiology. Feb 2013;118(2):409-415.
Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. Feb 2012;116(2):248-273.
Perlas A, Kirkham KR, Billing R, et al. The impact of analgesic modality on early ambulation following total knee arthroplasty. Reg Anesth Pain Med. Jul-Aug 2013;38(4):334-339.
Mudumbai SC, Kim TE, Howard SK, et al. Continuous adductor canal blocks are superior to continuous femoral nerve blocks in promoting early ambulation after TKA. Clin Orthop Relat Res. 2014 May;472(5):1377-83.
Edward R. Mariano, MD, MAS, FASA, FASRA is a physician specializing in anesthesiology, professor, husband, and father working to improve pain control, outcomes, and the overall experience for patients having surgery

 I came up with a short list of lessons that I’ve learned over the years. While some examples I included are anesthesiology-specific, the lessons themselves are not. Please feel free to edit, adapt, and add to this list; then disseminate it to the future physician leaders who will one day take our places.
I came up with a short list of lessons that I’ve learned over the years. While some examples I included are anesthesiology-specific, the lessons themselves are not. Please feel free to edit, adapt, and add to this list; then disseminate it to the future physician leaders who will one day take our places. We also don’t tend to do ourselves any favors. How many times have you heard someone say, “Hi I’m [first name only] with anesthesia”? According to the American Society of Anesthesiologists newsletter, approximately 60% of the public may not know that physician anesthesiologists go to medical school. While every member of the anesthesia care team plays a crucial role, the next level of non-physician provider in this model has one-tenth the amount of clinical training when compared to a physician anesthesiologist at graduation. I’ve written before about what I love about being an anesthesiologist, and being the physician whom patients trust to keep them safe during surgery is a privilege which comes with a great deal of responsibility.
We also don’t tend to do ourselves any favors. How many times have you heard someone say, “Hi I’m [first name only] with anesthesia”? According to the American Society of Anesthesiologists newsletter, approximately 60% of the public may not know that physician anesthesiologists go to medical school. While every member of the anesthesia care team plays a crucial role, the next level of non-physician provider in this model has one-tenth the amount of clinical training when compared to a physician anesthesiologist at graduation. I’ve written before about what I love about being an anesthesiologist, and being the physician whom patients trust to keep them safe during surgery is a privilege which comes with a great deal of responsibility. Thank your team. Taking the first steps on the path to leadership is not going to be easy. There will be many obstacles, not the least of which is time management. A high-functioning healthcare team of diverse backgrounds, skills, and abilities will accomplish much more than what an individual can do alone. Celebrate team wins. Respect each team member’s opinion even when it differs from yours.
Thank your team. Taking the first steps on the path to leadership is not going to be easy. There will be many obstacles, not the least of which is time management. A high-functioning healthcare team of diverse backgrounds, skills, and abilities will accomplish much more than what an individual can do alone. Celebrate team wins. Respect each team member’s opinion even when it differs from yours.







 re administering a medication, it’s not enough just to understand the complex pharmacologic effects of the drug and determine the right dose. The anesthesiologist also has to know how to dilute and prepare the drug, the appropriate route for the medication, which other medications are and are not compatible, and how to program the infusion device. In addition, an anesthesiologist has to be technically skilled at finding veins—sometimes in the hand or arm, sometimes leading centrally to the heart—in order to give the medication in the first place.
re administering a medication, it’s not enough just to understand the complex pharmacologic effects of the drug and determine the right dose. The anesthesiologist also has to know how to dilute and prepare the drug, the appropriate route for the medication, which other medications are and are not compatible, and how to program the infusion device. In addition, an anesthesiologist has to be technically skilled at finding veins—sometimes in the hand or arm, sometimes leading centrally to the heart—in order to give the medication in the first place.