Since 2012, the American Society of Anesthesiologists has promoted the Perioperative Surgical Home model in which anesthesiologists function as leaders in the coordination of perioperative care for surgical patients to improve outcomes (1,2). While anesthesiologists globally have had similar interests over the years, the unifying challenge continues to be the selection of outcomes and demonstration of improvement due to the anesthesiologist’s role and/or choice of anesthetic or analgesic technique. Since the types of outcomes and frequency of occurrence vary widely, a comprehensive discussion of perioperative outcomes is beyond the scope of this summary. Therefore, this review will focus on select anesthesiologist-driven factors related to acute pain management and anesthetic technique on perioperative outcomes and potential research directions.
Rare Outcomes and Big Data
For anesthesiologists, avoiding adverse events of the lowest frequency (death, recall, and nerve injury) receives highest priority with death ranking first among complications to avoid (3). Studies involving rare outcomes, positive or negative, will invariably require accumulation of “big data.” Such studies must either involve multiple institutions over a long study period (if prospective) or access data involving a large cohort of patients for retrospective studies; these study designs involving longitudinal data may also require advanced statistical methods (4). For example, Memtsoudis and colleagues sought to evaluate postoperative morbidity and mortality for lower extremity joint arthroplasty patients in a recent study (5). They utilized a large nationwide administrative database maintained by Premier Perspective, Inc. (Charlotte, NC, USA); the study data were gathered from 382,236 patients in approximately 400 acute care hospitals throughout the United States over 4 years (5). Other retrospective cohort studies comparing the occurrence of perioperative complications such as surgical site infections, cardiopulmonary morbidity, and mortality have used the American College of Surgeons National Surgical Quality Improvement Project (NSQIP) (6-8). NSQIP originally started within the Veterans Health Administration (VHA) system in the 1980s with a small sample of hospitals; this project, which included public reporting of outcomes data, eventually expanded to include all VHA surgical facilities and others outside the VHA system (9). Multi-center prospective registries such as the SOS Regional Anesthesia Hotline (10, 11) and AURORA (12, 13) have been developed for outcomes research and have reported the occurrence rates of rare complications related to regional anesthesia. The disadvantages to these data-driven studies include lack or randomization introducing potential bias, missing or incorrectly coded data, inability to draw conclusions regarding causation, and restrictions to access such as information security issues and/or cost (e.g., the Premier database). However, these retrospective cohort database studies may offer large samples sizes and administrative data from actual “real world” patients over a longer period of time and may identify important associations that influence clinical practice and generate hypotheses for future prospective studies.
Anesthesia Type and Perioperative Mortality
Based on the study by Memtsoudis and colleagues, overall 30-day mortality for lower extremity arthroplasty patients is lower for patients who receive neuraxial and combined neuraxial-general anesthesia compared to general anesthesia alone (5). In most categories, the rates of occurrence of in-hospital complications are also lower for the neuraxial and combined neuraxial-general anesthesia groups vs. the general anesthesia group, and transfusion requirements are lowest for the neuraxial group compared to all other groups (5). Studies using NSQIP have reported no difference in 30-day mortality for carotid endarterectomy patients associated with anesthetic technique although regional anesthesia patients are more likely to have a shorter operative time and next-day discharge (8); similarly, there is no difference in 30-day mortality for endovascular aortic aneurysm repair although general anesthesia patients are more likely to have longer length of stay and pulmonary complications (14).
Perioperative Analgesia and Cancer Recurrence
In a relatively-small matched retrospective study, Exadaktylos and colleagues have reported lower rates of recurrence and metastasis for breast cancer surgery patients who receive paravertebral analgesia vs. conventional systemic opioids (15). Although the exact mechanism was not well-understood at that time (regional anesthesia vs. reduction in the use of anesthetic agents and opioids), clinical and basic science research in this area has grown rapidly and has demonstrated mixed results. A follow-up study involving 503 patients who underwent abdominal surgery for cancer and were previously enrolled in a large multi-center clinical trial (16) and a retrospective database study of 424 colorectal cancer patients who underwent laparoscopic resection (17) have not shown a difference in recurrence-free survival or mortality. A recent meta-analysis including 14 prospective and retrospective studies involving cancer patients (colorectal, ovarian, breast, prostate, and hepatocellular) demonstrates a positive association between epidural analgesia and overall survival but no difference in recurrence-free survival compared to general anesthesia with opioid analgesia (18).
Analgesic Technique and Persistent Postsurgical Pain
Chronic pain may develop after many common operations including breast surgery, hernia repair, thoracic surgery, and amputation and is associated with severe acute pain in the postoperative period (19). While regional analgesic techniques are effective for acute pain management, currently-available data are inconclusive with regard to their ability to prevent the development of persistent postsurgical pain (20-22). There is an opportunity to use larger databases to investigate this issue further.
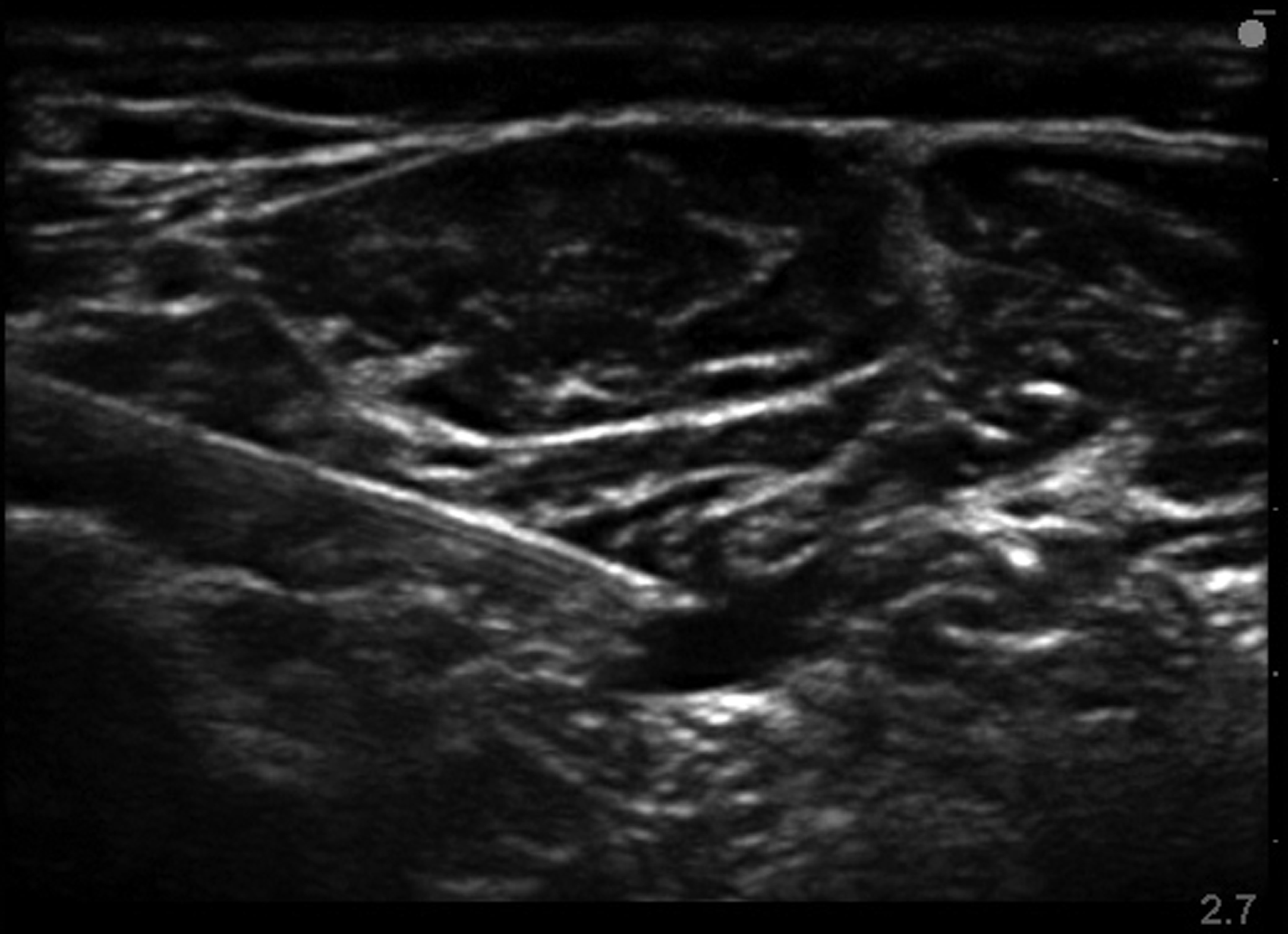
Ultrasound and Patient Safety
In 2010, the American Society of Regional Anesthesia and Pain Medicine published a series of articles presenting the evidence basis for ultrasound in regional anesthesia (23). According to the article focused on patient safety, evidence at the time suggested that ultrasound may decrease the incidence of minor adverse events (e.g., hemidiaphragmatic paresis from interscalene block or inadvertent vascular puncture), but serious complications such as local anesthetic systemic toxicity (LAST) and nerve injury did not occur at different rates based on the nerve localization technique (24). Since then, a large prospective multi-center registry study has shown that the use of ultrasound in regional anesthesia does reduce the incidence of LAST compared to traditional techniques (13). Similar methodology may be applied to other rare complications associated with anesthetic interventions.
Perioperative Medicine and Health Care Costs
Approximately 31% of costs related to inpatient perioperative care is attributable to the ward admission (25). Anesthesiologists as perioperative physicians have an opportunity to influence the cost of surgical care by decreasing hospital length of stay through effective pain management and by developing coordinated multi-disciplinary clinical pathways (26, 27).
REFERENCES
- Vetter TR, Goeddel LA, Boudreaux AM, Hunt TR, Jones KA, Pittet JF. The Perioperative Surgical Home: how can it make the case so everyone wins? BMC anesthesiology. 2013;13:6.
- Vetter TR, Ivankova NV, Goeddel LA, McGwin G, Jr., Pittet JF. An Analysis of Methodologies That Can Be Used to Validate if a Perioperative Surgical Home Improves the Patient-centeredness, Evidence-based Practice, Quality, Safety, and Value of Patient Care. Anesthesiology. Dec 2013;119(6):1261-1274.
- Macario A, Weinger M, Truong P, Lee M. Which clinical anesthesia outcomes are both common and important to avoid? The perspective of a panel of expert anesthesiologists. Anesth Analg. May 1999;88(5):1085-1091.
- Ma Y, Mazumdar M, Memtsoudis SG. Beyond repeated-measures analysis of variance: advanced statistical methods for the analysis of longitudinal data in anesthesia research. Reg Anesth Pain Med. Jan-Feb 2012;37(1):99-105.
- Memtsoudis SG, Sun X, Chiu YL, et al. Perioperative comparative effectiveness of anesthetic technique in orthopedic patients. Anesthesiology. May 2013;118(5):1046-1058.
- Liu J, Ma C, Elkassabany N, Fleisher LA, Neuman MD. Neuraxial anesthesia decreases postoperative systemic infection risk compared with general anesthesia in knee arthroplasty. Anesth Analg. Oct 2013;117(4):1010-1016.
- Radcliff TA, Henderson WG, Stoner TJ, Khuri SF, Dohm M, Hutt E. Patient risk factors, operative care, and outcomes among older community-dwelling male veterans with hip fracture. J Bone Joint Surg Am. Jan 2008;90(1):34-42.
- Schechter MA, Shortell CK, Scarborough JE. Regional versus general anesthesia for carotid endarterectomy: the American College of Surgeons National Surgical Quality Improvement Program perspective. Surgery. Sep 2012;152(3):309-314.
- Ingraham AM, Richards KE, Hall BL, Ko CY. Quality improvement in surgery: the American College of Surgeons National Surgical Quality Improvement Program approach. Advances in surgery. 2010;44:251-267.
- Auroy Y, Benhamou D, Bargues L, et al. Major complications of regional anesthesia in France: The SOS Regional Anesthesia Hotline Service. Anesthesiology. Nov 2002;97(5):1274-1280.
- Auroy Y, Narchi P, Messiah A, Litt L, Rouvier B, Samii K. Serious complications related to regional anesthesia: results of a prospective survey in France. Anesthesiology. Sep 1997;87(3):479-486.
- Barrington MJ, Watts SA, Gledhill SR, et al. Preliminary results of the Australasian Regional Anaesthesia Collaboration: a prospective audit of more than 7000 peripheral nerve and plexus blocks for neurologic and other complications. Reg Anesth Pain Med. Nov-Dec 2009;34(6):534-541.
- Barrington MJ, Kluger R. Ultrasound guidance reduces the risk of local anesthetic systemic toxicity following peripheral nerve blockade. Reg Anesth Pain Med. Jul-Aug 2013;38(4):289-297.
- Edwards MS, Andrews JS, Edwards AF, et al. Results of endovascular aortic aneurysm repair with general, regional, and local/monitored anesthesia care in the American College of Surgeons National Surgical Quality Improvement Program database. J Vasc Surg. Nov 2011;54(5):1273-1282.
- Exadaktylos AK, Buggy DJ, Moriarty DC, Mascha E, Sessler DI. Can anesthetic technique for primary breast cancer surgery affect recurrence or metastasis? Anesthesiology. Oct 2006;105(4):660-664.
- Myles PS, Peyton P, Silbert B, Hunt J, Rigg JR, Sessler DI. Perioperative epidural analgesia for major abdominal surgery for cancer and recurrence-free survival: randomised trial. BMJ. 2011;342:d1491.
- Day A, Smith R, Jourdan I, Fawcett W, Scott M, Rockall T. Retrospective analysis of the effect of postoperative analgesia on survival in patients after laparoscopic resection of colorectal cancer. Br J Anaesth. Aug 2012;109(2):185-190.
- Chen WK, Miao CH. The effect of anesthetic technique on survival in human cancers: a meta-analysis of retrospective and prospective studies. PloS one. 2013;8(2):e56540.
- Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. May 13 2006;367(9522):1618-1625.
- Kairaluoma PM, Bachmann MS, Rosenberg PH, Pere PJ. Preincisional paravertebral block reduces the prevalence of chronic pain after breast surgery. Anesth Analg. Sep 2006;103(3):703-708.
- Schnabel A, Reichl SU, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of paravertebral blocks in breast surgery: a meta-analysis of randomized controlled trials. Br J Anaesth. Dec 2010;105(6):842-852.
- Wildgaard K, Ravn J, Kehlet H. Chronic post-thoracotomy pain: a critical review of pathogenic mechanisms and strategies for prevention. Eur J Cardiothorac Surg. Jul 2009;36(1):170-180.
- Neal JM, Brull R, Chan VW, et al. The ASRA evidence-based medicine assessment of ultrasound-guided regional anesthesia and pain medicine: Executive summary. Reg Anesth Pain Med. Mar-Apr 2010;35(2 Suppl):S1-9.
- Neal JM. Ultrasound-guided regional anesthesia and patient safety: An evidence-based analysis. Reg Anesth Pain Med. Mar-Apr 2010;35(2 Suppl):S59-67.
- Macario A, Vitez TS, Dunn B, McDonald T. Where are the costs in perioperative care? Analysis of hospital costs and charges for inpatient surgical care. Anesthesiology. Dec 1995;83(6):1138-1144.
- Ilfeld BM, Mariano ER, Williams BA, Woodard JN, Macario A. Hospitalization costs of total knee arthroplasty with a continuous femoral nerve block provided only in the hospital versus on an ambulatory basis: a retrospective, case-control, cost-minimization analysis. Reg Anesth Pain Med. Jan-Feb 2007;32(1):46-54.
- Jakobsen DH, Sonne E, Andreasen J, Kehlet H. Convalescence after colonic surgery with fast-track vs conventional care. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. Oct 2006;8(8):683-687.
Facebook
LinkedIn
Pinterest
E-mail
Related Posts:









 Many people, even those who work in the operating room every day, take safe anesthesia care for granted. There has been growing pressure recently to abandon the team model and remove physician anesthesiologists’ supervision of nurse anesthetists with the latest threat coming from within
Many people, even those who work in the operating room every day, take safe anesthesia care for granted. There has been growing pressure recently to abandon the team model and remove physician anesthesiologists’ supervision of nurse anesthetists with the latest threat coming from within