 Among Medicare beneficiaries in the United States, the number of primary total knee arthroplasty (TKA) procedures from 1991 to 2010 increased by 161.5% (1). Postoperative pain remains one of patients’ top concerns when undergoing elective surgery (2) and can limit patients’ functional ability in the early postoperative period (3). Providing effective perioperative pain control has potential longer-term implications since early rehabilitation may lead to improvements in functional outcomes later on (4). With the ability to select specific targets for local anesthetic injection and infusion, regional anesthesia techniques, neuraxial and peripheral, are commonly included in the perioperative analgesic protocol for joint arthroplasty patients (5-11). While the data supporting the analgesic efficacy of regional anesthesia techniques in this setting are strongly positive, studies attempting to attribute functional outcome benefits to regional anesthesia demonstrate mixed results.
Among Medicare beneficiaries in the United States, the number of primary total knee arthroplasty (TKA) procedures from 1991 to 2010 increased by 161.5% (1). Postoperative pain remains one of patients’ top concerns when undergoing elective surgery (2) and can limit patients’ functional ability in the early postoperative period (3). Providing effective perioperative pain control has potential longer-term implications since early rehabilitation may lead to improvements in functional outcomes later on (4). With the ability to select specific targets for local anesthetic injection and infusion, regional anesthesia techniques, neuraxial and peripheral, are commonly included in the perioperative analgesic protocol for joint arthroplasty patients (5-11). While the data supporting the analgesic efficacy of regional anesthesia techniques in this setting are strongly positive, studies attempting to attribute functional outcome benefits to regional anesthesia demonstrate mixed results.
The main challenge in assessing functional outcomes following joint replacement is the selection of outcomes; these can be divided into performance-based outcomes and self-reported outcomes (12, 13). Performance-based outcomes are measurable and arguably more objective, although often subject to effort. Examples of these outcomes and their units of measure include joint range of motion in degrees (e.g., flexion, extension, rotation); timed walking tests in meters (e.g., 6 minute walking test [6MWT], 2 minute walking test [2MWT]); muscle strength in units of force using a dynamometer (e.g., maximum voluntary isometric contraction [MVIC]); and timed up-and-go (TUG) in minutes (12, 13). Self-reported outcomes are typically survey-based; examples include the Western Ontario McMaster Universities Osteoarthritis Index (WOMAC), Knee Society Score, and Lower Extremity Functional Scale (12, 13). Since patient perception of successful rehabilitation is an important factor, self-reported outcomes should be reported with performance-based outcomes (12). Another important challenge when measuring and comparing functional outcomes is that clinical pathways for joint arthroplasty that integrate pain management (including regional analgesia), physical therapy, nursing, and surgical care are often specific to individual institutions, and institutions may vary with respect to rehabilitation goals and the timeline to achieve them.
Epidural Analgesia
Epidural analgesia has been used for perioperative pain management in joint replacement patients since at least the 1980s (14, 15). In 1987, Raj and colleagues compared postoperative systemic opioid analgesia to continuous epidural analgesia (bupivacaine 0.25% at 6-15 ml/hr) for TKA patients in a prospective non-randomized study (14). Although pain scores were lower in the epidural group, not surprisingly a high proportion of these patients experienced complete motor block of the lower extremities; although the authors mention “rigorous passive exercises,” specific rehabilitation outcomes were not reported (14). Later studies have reported functional benefits associated with continuous epidural analgesia, such as shorter time to achieve ambulation distance and range of motion goals, when compared to parenteral opioids alone (16). At institutions where continuous epidural analgesia is currently employed as part of a multimodal analgesic protocol, very low doses of local anesthetic (e.g., 0.06% bupivacaine) in combination with opioid are used in order to minimize motor block (17).
Peripheral Nerve Blocks
The innervation of the knee is complex and involves contributions from both the lumbar and sacral plexuses. While epidural analgesia is effective, it is also associated with clinically-significant side effects (e.g., nausea/vomiting and motor block of the non-operative limb) (5, 18) and the potential for neuraxial hematoma in patients on pharmacologic thromboprophylaxis (19). Thus, peripheral nerve block options, either single-injection or continuous infusions, have been explored for postoperative pain management.
Two early studies by Capdevila (6) and Singelyn (20) have shown continuous femoral nerve block (FNB) to provide comparable analgesia and physical therapy outcome achievement with fewer side effects when compared to epidural analgesia. Both of these studies also demonstrated shorter hospital length of stay for the regional anesthesia groups compared to an opioid-only group (6, 20), but hospitalization duration for these studies was, on average, greater than what has been reported in other studies (21). Triple-masked, placebo-controlled randomized clinical trials have shown that CPNB can shorten the time to achieve discharge criteria, including 100 m ambulation distance, for TKA (10, 22) and total hip arthroplasty (THA) (9) patients, but actual hospital duration was similar in these studies.
One of the interesting findings from the Singelyn study was that regional anesthesia patients maintained a knee flexion advantage over the opioid-only group at 6 week follow-up (20); although this advantage did not remain at 3 months, this finding supported the potential for long-term functional improvement resulting from effective pain management and early rehabilitation in the immediate perioperative period (4). In a randomized comparison of continuous FNB to local infiltration analgesia (LIA) for TKA, the FNB group spent more time out of bed walking; at 6 weeks, the FNB group showed more improvement in performance-based (6MWT) and self-reported functional outcome assessments (23). In contrast, the one year follow-up studies of randomized clinical trial subjects (9, 10, 22) using self-reported outcome measures for functional status (WOMAC) did not show long-term improvement associated with regional anesthesia techniques (24-27).
The rehabilitation outcome measured in the immediate postoperative period that correlates best with long-term functional improvement is not yet established. Ambulation distance is often measured by physical therapists and included in discharge criteria (9, 10, 22). For institutions that emphasize ambulation in their clinical pathway for lower extremity joint arthroplasty, a major concern raised with regard to FNBs is the potential association with increased fall risk (28, 29) although a recent large database study disputes this finding. In-hospital falls can lead to prolonged hospital stays with higher costs and are associated with more frequent postoperative complications, including serious organ system dysfunction and death (30). With currently-available local anesthetic solutions and typical doses, perineural infusion does produce clinically-significant quadriceps weakness when administered near the femoral nerve or lumbar plexus (31, 32). Since the local anesthetics themselves cannot select sensory over motor nerves( 33), anesthesiologists have started exploring alternate nerve block locations to minimize the risk of motor block and maximize patient rehabilitation.
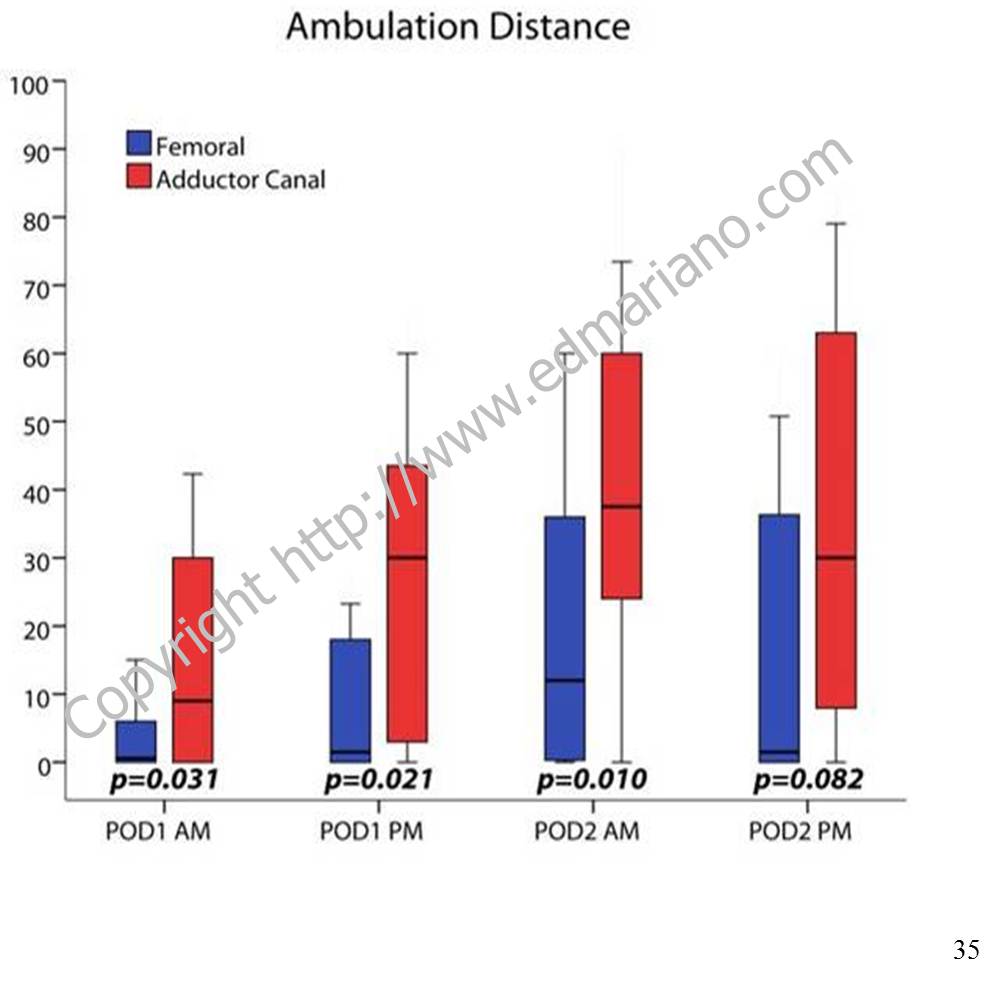
For TKA, a more distal nerve block location in the adductor canal can provide effective analgesia postoperatively (34) and has been shown to better preserve quadriceps strength compared to a FNB in both volunteers (35) and clinical patients (11). Regional analgesic techniques are only one part of the overall pain management plan. While they are often included in multimodal analgesic protocols along with non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and low-dose opioids (36), there is a growing body of evidence to support the adductor canal block as the regional analgesic technique of choice for promoting postoperative ambulation within a clinical pathway (37, 38).
For patient information with answers to frequently-asked questions about regional anesthesia, please see “Regional Anesthesia FAQs.”
References
- Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991-2010. JAMA. Sep 26 2012;308(12):1227-1236.
- Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg. Sep 1999;89(3):652-658.
- Holm B, Kristensen MT, Myhrmann L, et al. The role of pain for early rehabilitation in fast track total knee arthroplasty. Disability and rehabilitation. 2010;32(4):300-306.
- Munin MC, Rudy TE, Glynn NW, Crossett LS, Rubash HE. Early inpatient rehabilitation after elective hip and knee arthroplasty. JAMA. Mar 18 1998;279(11):847-852.
- Barrington MJ, Olive D, Low K, Scott DA, Brittain J, Choong P. Continuous femoral nerve blockade or epidural analgesia after total knee replacement: a prospective randomized controlled trial. Anesth Analg. Dec 2005;101(6):1824-1829.
- Capdevila X, Barthelet Y, Biboulet P, Ryckwaert Y, Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology. Jul 1999;91(1):8-15.
- Chelly JE, Greger J, Gebhard R, et al. Continuous femoral blocks improve recovery and outcome of patients undergoing total knee arthroplasty. J Arthroplasty. Jun 2001;16(4):436-445.
- Hebl JR, Dilger JA, Byer DE, et al. A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. Reg Anesth Pain Med. Nov-Dec 2008;33(6):510-517.
- Ilfeld BM, Ball ST, Gearen PF, et al. Ambulatory continuous posterior lumbar plexus nerve blocks after hip arthroplasty: a dual-center, randomized, triple-masked, placebo-controlled trial. Anesthesiology. Sep 2008;109(3):491-501.
- Ilfeld BM, Le LT, Meyer RS, et al. Ambulatory continuous femoral nerve blocks decrease time to discharge readiness after tricompartment total knee arthroplasty: a randomized, triple-masked, placebo-controlled study. Anesthesiology. Apr 2008;108(4):703-713.
- Jaeger P, Zaric D, Fomsgaard JS, et al. Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: a randomized, double-blind study. Reg Anesth Pain Med. Nov-Dec 2013;38(6):526-532.
- Choi S, Trang A, McCartney CJ. Reporting functional outcome after knee arthroplasty and regional anesthesia: a methodological primer. Reg Anesth Pain Med. Jul-Aug 2013;38(4):340-349.
- Bernucci F, Carli F. Functional outcome after major orthopedic surgery: the role of regional anesthesia redefined. Curr Opin Anaesthesiol. Oct 2012;25(5):621-628.
- Raj PP, Knarr DC, Vigdorth E, et al. Comparison of continuous epidural infusion of a local anesthetic and administration of systemic narcotics in the management of pain after total knee replacement surgery. Anesth Analg. May 1987;66(5):401-406.
- Pettine KA, Wedel DJ, Cabanela ME, Weeks JL. The use of epidural bupivacaine following total knee arthroplasty. Orthopaedic review. Aug 1989;18(8):894-901.
- Mahoney OM, Noble PC, Davidson J, Tullos HS. The effect of continuous epidural analgesia on postoperative pain, rehabilitation, and duration of hospitalization in total knee arthroplasty. Clin Orthop Relat Res. Nov 1990(260):30-37.
- YaDeau JT, Cahill JB, Zawadsky MW, et al. The effects of femoral nerve blockade in conjunction with epidural analgesia after total knee arthroplasty. Anesth Analg. Sep 2005;101(3):891-895, table of contents.
- Zaric D, Boysen K, Christiansen C, Christiansen J, Stephensen S, Christensen B. A comparison of epidural analgesia with combined continuous femoral-sciatic nerve blocks after total knee replacement. Anesth Analg. Apr 2006;102(4):1240-1246.
- Horlocker TT, Wedel DJ, Rowlingson JC, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Reg Anesth Pain Med. Jan-Feb 2010;35(1):64-101.
- Singelyn FJ, Deyaert M, Joris D, Pendeville E, Gouverneur JM. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous three-in-one block on postoperative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg. Jul 1998;87(1):88-92.
- Salinas FV, Liu SS, Mulroy MF. The effect of single-injection femoral nerve block versus continuous femoral nerve block after total knee arthroplasty on hospital length of stay and long-term functional recovery within an established clinical pathway. Anesth Analg. Apr 2006;102(4):1234-1239.
- Ilfeld BM, Mariano ER, Girard PJ, et al. A multicenter, randomized, triple-masked, placebo-controlled trial of the effect of ambulatory continuous femoral nerve blocks on discharge-readiness following total knee arthroplasty in patients on general orthopaedic wards. Pain. Sep 2010;150(3):477-484.
- Carli F, Clemente A, Asenjo JF, et al. Analgesia and functional outcome after total knee arthroplasty: periarticular infiltration vs continuous femoral nerve block. Br J Anaesth. Aug 2010;105(2):185-195.
- Ilfeld BM, Shuster JJ, Theriaque DW, et al. Long-term pain, stiffness, and functional disability after total knee arthroplasty with and without an extended ambulatory continuous femoral nerve block: a prospective, 1-year follow-up of a multicenter, randomized, triple-masked, placebo-controlled trial. Reg Anesth Pain Med. Mar-Apr 2011;36(2):116-120.
- Morin AM, Kratz CD, Eberhart LH, et al. Postoperative analgesia and functional recovery after total-knee replacement: comparison of a continuous posterior lumbar plexus (psoas compartment) block, a continuous femoral nerve block, and the combination of a continuous femoral and sciatic nerve block. Reg Anesth Pain Med. Sep-Oct 2005;30(5):434-445.
- Ilfeld BM, Ball ST, Gearen PF, et al. Health-related quality of life after hip arthroplasty with and without an extended-duration continuous posterior lumbar plexus nerve block: a prospective, 1-year follow-up of a randomized, triple-masked, placebo-controlled study. Anesth Analg. Aug 2009;109(2):586-591.
- Ilfeld BM, Meyer RS, Le LT, et al. Health-related quality of life after tricompartment knee arthroplasty with and without an extended-duration continuous femoral nerve block: a prospective, 1-year follow-up of a randomized, triple-masked, placebo-controlled study. Anesth Analg. Apr 2009;108(4):1320-1325.
- Feibel RJ, Dervin GF, Kim PR, Beaule PE. Major complications associated with femoral nerve catheters for knee arthroplasty: a word of caution. J Arthroplasty. Sep 2009;24(6 Suppl):132-137.
- Ilfeld BM, Duke KB, Donohue MC. The association between lower extremity continuous peripheral nerve blocks and patient falls after knee and hip arthroplasty. Anesth Analg. Dec 2010;111(6):1552-1554.
- Memtsoudis SG, Dy CJ, Ma Y, Chiu YL, Della Valle AG, Mazumdar M. In-hospital patient falls after total joint arthroplasty: incidence, demographics, and risk factors in the United States. J Arthroplasty. Jun 2012;27(6):823-828 e821.
- Charous MT, Madison SJ, Suresh PJ, et al. Continuous femoral nerve blocks: varying local anesthetic delivery method (bolus versus basal) to minimize quadriceps motor block while maintaining sensory block. Anesthesiology. Oct 2011;115(4):774-781.
- Ilfeld BM, Moeller LK, Mariano ER, et al. Continuous peripheral nerve blocks: is local anesthetic dose the only factor, or do concentration and volume influence infusion effects as well? Anesthesiology. Feb 2010;112(2):347-354.
- Ilfeld BM, Yaksh TL. The end of postoperative pain–a fast-approaching possibility? And, if so, will we be ready? Reg Anesth Pain Med. Mar-Apr 2009;34(2):85-87.
- Lund J, Jenstrup MT, Jaeger P, Sorensen AM, Dahl JB. Continuous adductor-canal-blockade for adjuvant post-operative analgesia after major knee surgery: preliminary results. Acta Anaesthesiol Scand. Jan 2011;55(1):14-19.
- Jaeger P, Nielsen ZJ, Henningsen MH, Hilsted KL, Mathiesen O, Dahl JB. Adductor Canal Block versus Femoral Nerve Block and Quadriceps Strength: A Randomized, Double-blind, Placebo-controlled, Crossover Study in Healthy Volunteers. Anesthesiology. Feb 2013;118(2):409-415.
- Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. Feb 2012;116(2):248-273.
- Perlas A, Kirkham KR, Billing R, et al. The impact of analgesic modality on early ambulation following total knee arthroplasty. Reg Anesth Pain Med. Jul-Aug 2013;38(4):334-339.
- Mudumbai SC, Kim TE, Howard SK, et al. Continuous adductor canal blocks are superior to continuous femoral nerve blocks in promoting early ambulation after TKA. Clin Orthop Relat Res. 2014 May;472(5):1377-83.



 The application cycle for the 2014-15 Stanford Regional Anesthesiology and Acute Pain Medicine Fellowship class is still open for 1 off-cycle spot scheduled to start in Winter 2015. The application cycle for 2015-16 is also open now and will remain open until Summer 2014.
The application cycle for the 2014-15 Stanford Regional Anesthesiology and Acute Pain Medicine Fellowship class is still open for 1 off-cycle spot scheduled to start in Winter 2015. The application cycle for 2015-16 is also open now and will remain open until Summer 2014.