As an anesthesiologist, I am a physician who cares for patients when they are most vulnerable. Under anesthesia, no one is able to call for help. Every day patients have surgery in operating rooms all over the world, and it is the job of the physician anesthesiologist to watch over them, monitor their bodies’ responses to stress, breathe for them, provide them with pain relief, and fight for them when unexpected crises occur. It is my job to calm the fears of my patients and families, listen to their requests, manage their expectations, and develop a plan that will provide them with the best outcome after surgery.
My belief in this connection between physicians, patients, and families as an anesthesiologist stretches into my administrative roles as well. As Chief of the Anesthesiology and Perioperative Care Service and Associate Chief of Staff for Inpatient Surgical Services at the VA Palo Alto Health Care System (VAPAHCS), I am grateful for the opportunity to work with an incredible team of physicians, respiratory therapists, surgeons, advanced practice providers, technicians, and administrative staff members who are focused on our mission to provide the highest quality Veteran-centered care by leading, educating, and innovating in anesthesiology and perioperative medicine.
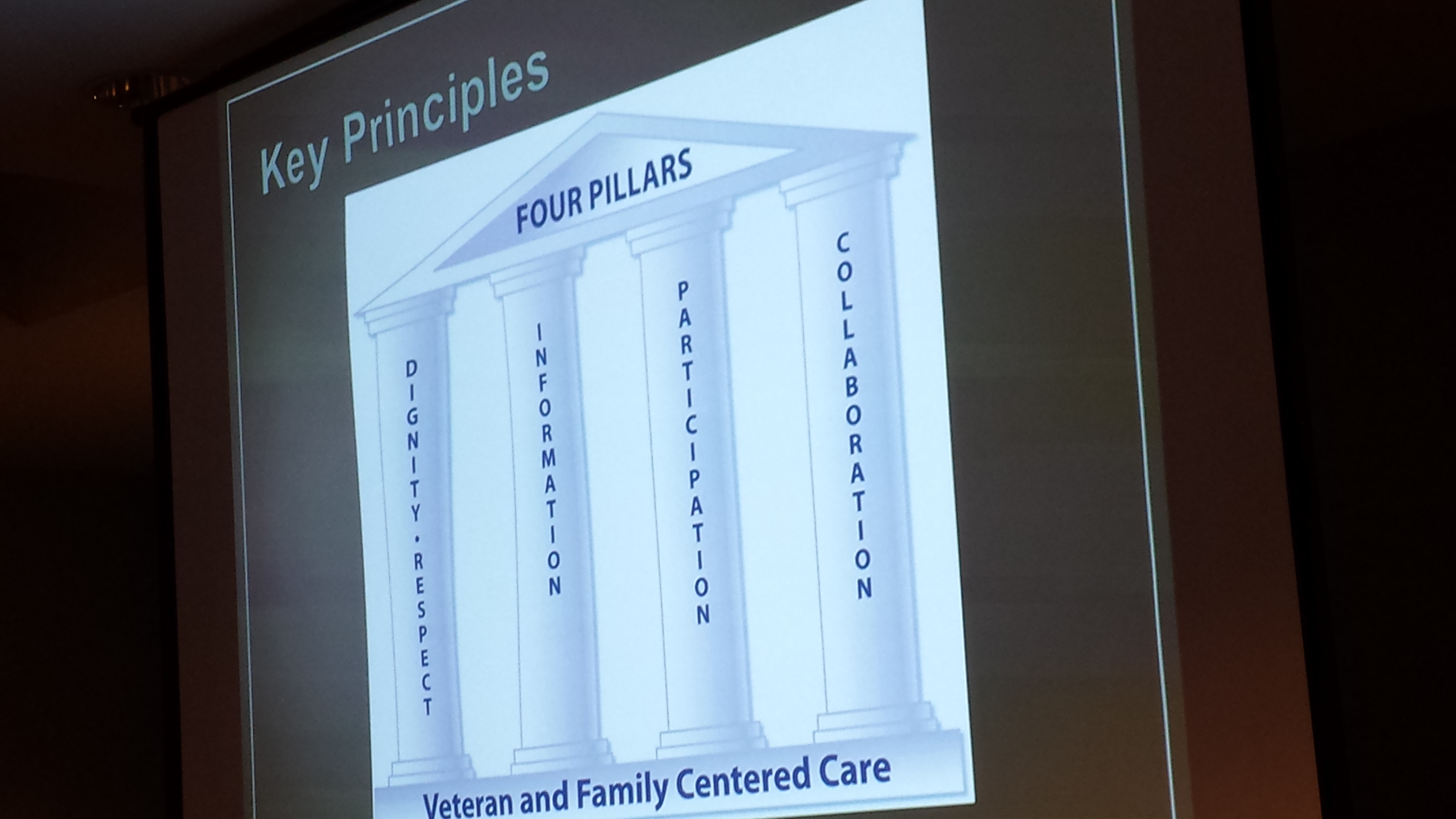
In order to accomplish this mission, we need the best information available to guide our decisions and a diversity of perspectives to enhance our ability to train new clinicians and explore relevant research questions. We have been fortunate to partner with our friends and colleagues in the Veteran and Family Advisory Council (VFAC) on a number of exciting projects. First, our Service manages the simulation center at VAPAHCS and is responsible for coordinating simulation-based training for all clinicians. Members of VFAC have been directly involved in simulation activities, even taking on active roles as the patient or family member in standardized training scenarios, to help us educate clinicians from various disciplines and all training levels. Debriefing after these simulation exercises gives our clinical trainees and practicing clinicians the unique perspective of real patients and family members which is essential to their professional development as modern medicine continues to progress towards a model of patient-centered care.
Once a year, our Service organizes a faculty development retreat during which we reassess our mission, vision, strategic priorities, and tactics and work on one or two big ideas. Two years ago in 2015, we invited our VFAC partners to join us at our annual retreat to brainstorm improvement ideas related to patient-centered care in the perioperative environment, intensive care unit, and pain management. The general theme of the retreat addressed public perception and professional reputation of anesthesiologists and the specialty of anesthesiology. Having members of VFAC present at the retreat to share their knowledge, opinions, and questions has inspired a few subsequent improvement activities and other projects to enhance the range of services that we provide to our patients and their families.
Finally, working together with VFAC, and knowing members personally, has allowed our clinical Service to solicit feedback on a regular basis. Not all hospitals enjoy the level of access to a community of engaged patients and families like we do at VAPAHCS. When we revised our preoperative education materials for patients, we went to VFAC for input. When we were critically reviewing our website to update our online patient educational materials on anesthesia and perioperative care, we presented at the VFAC meeting to get the members’ feedback and suggestions. With their help, we have been able to improve the accessibility and readability of our online content and provide our patients and their families with useful information that can help prepare them for surgery.
We are very grateful to VFAC for its priceless contributions to our healthcare system, our patients, and our Service. We look forward to continued collaboration on future projects!
This blog has also appeared as a featured story on the VA Palo Alto Health Care System website.
Many people, even those who work in the operating room every day, take safe anesthesia care for granted. There has been growing pressure recently to abandon the team model and remove physician anesthesiologists’ supervision of nurse anesthetists with the latest threat coming from within Veterans Affairs (VA) healthcare. For our Veterans, our heroes and arguably some of the most medically complex patients, having both physician anesthesiologists and nurse anesthetists working together as a team makes sense.
Having a team with members who train differently and have different perspectives can only benefit the patient; physician anesthesiologists draw on their medical training while nurse anesthetists bring valuable nursing experience. Providing anesthesia is often compared to flying a passenger airplane, and the care team model is like having both a pilot and a co-pilot. Has flying become so safe that we no longer need the pilot? Seconds count in flight, and they count in the operating room when a patient’s life is on the line. If approved, the proposed change in the VA nursing handbook will abolish this team model without giving Veterans a choice and will require VA hospitals to assign Veterans having surgery either a nurse anesthetist OR a physician anesthesiologist but not offer both. If they were given the choice, however, I think our Veterans would choose “AND” instead of “OR.” We all should. In case a crisis happens during surgery, every patient should have access to a physician anesthesiologist.
Not too long ago operating room personnel had to worry about explosive anesthetic gases, and patients faced the risk of developing organ failure after every time they had anesthesia in addition to the usual perils of having surgery. This changed when anesthesiology became a medical specialty and profession for physicians.
How is anesthesiology different than anesthesia? Anesthesia, a word with Greek origin, means “without sensation.” Often referred to as “going to sleep,” general anesthesia is more like a complex drug-induced coma that can still carry serious risk, and a person’s physical and emotional reactions to anesthetic agents are not always predictable.
Anesthesiologyis a science like biology or physiology and a specialty field of medicine like cardiology or radiology. Modern anesthesiologists are physicians, scientists, educators, and patient safety advocates. The heart of anesthesiology continues to be the patient experience. As physician anesthesiologists, we specialize in relieving anxiety, preventing and treating pain, preventing and managing complications related to surgery, and improving the outcomes for patients who undergo invasive procedures. The average physician anesthesiologist spends nearly a decade in postgraduate education after college and logs 16,000 hours of clinical training to learn to apply the best available evidence in clinical practice. Academic physicians and scientists focused on anesthesiology are responsible for the discovery of the newer and safer anesthetic and analgesic agents we use every day.
Anesthesia administration by non-physicians such as nurse anesthetists and certified anesthesiologist assistants is supported by the American Society of Anesthesiologists within the physician-led anesthesia care team model. A similar model is used in the intensive care unit with physician intensivists supervising teams that include acute care nurse practitioners. To preserve safe, high-quality physician-led anesthesia care for our nation’s Veterans, please support the team model and #SafeVACare by speaking up on http://www.safevacare.org by July 25th. It only takes a minute to post a comment, but the consequences of not saying something may be serious and long-lasting.
Healthcare around the world is changing. In the United States, healthcare reform has been focused on achieving the “triple aim” as described by Berwick (1). This triple aim encompasses 3 goals: improving the patient experience, reducing costs of care, and improving population health. The Perioperative Surgical Home (PSH) is a conceptual model introduced by the American Society of Anesthesiologists (ASA) in the past 5 years that may serve as an integrator to help hospitals achieve the triple aim (2). PSH is defined as “a patient-centered, physician anesthesiologist-led, multidisciplinary team-based practice model that coordinates surgical patient care throughout the continuum from the decision to pursue surgery through convalescence” (3). In reality, a PSH can take many forms, and the concept is analogous to the “Perioperative Medicine: the Pathway to Better Surgical Care” initiative by the Royal College of Anaesthetists in the United Kingdom. To date, there have been few published descriptions of actual PSH programs.
Pain medicine is woven throughout the three main elements of the PSH: preoperative preparation, intraoperative care, and postoperative recovery and rehabilitation (4). Preoperatively, anesthesiologists and pain medicine specialists have an opportunity to influence patient care by identifying patients who are considered high risk for surgery and tailor an individualized preoperative preparation plan for them. For example, the patient with chronic pain treated with long-acting opioids may benefit from optimizing the preoperative analgesic medication regimen, even tapering the opioid dose, or prescribing cognitive, behavioral, or physical therapy prior to elective major surgery like lower extremity joint replacement. During the intraoperative period, anesthetic protocols provide consistent care for surgical patients, and implementing clinical pathways that include regional anesthesia techniques have been shown to decrease perioperative opioid use and improve outcomes. For patients who have surgery, pain has a profound influence on the hospital experience. In the United States, the patient experience of care is one of three domains that influence hospital incentive payment amounts from the Center for Medicare and Medicaid Services. Patient experience is assessed using a survey, and 7 of 32 questions directly or indirectly relate to pain management (5). After the immediate postoperative period, integrated pain management can help patients achieve physical therapy goals and facilitate the transition to after-hospital rehabilitation. For challenging patients with chronic pain, this process may require careful coordination between the in-hospital anesthesiologist, outpatient pain clinic physician, and primary care physician (4).
The practice of anesthesiology in the United States is evolving, and there is a greater emphasis on demonstrating value. Anesthesiologists have historically been successful in establishing perioperative clinical pathways that improve acute pain management especially in orthopedic surgery, and setting up regional anesthesia and acute pain medicine programs has played a key role (6). However, competing priorities require revision of clinical pathways from time to time. For example, concerns regarding quadriceps muscle weakness with femoral nerve blocks (7) and the potential for falls (8) have led to innovations in selective nerve block techniques for knee replacement patients (9) and greater achievements in functional rehabilitation (10). By establishing a PSH model, anesthesiologists have greater opportunity but also greater responsibility for reducing perioperative complications that may or may not typically be considered within the realm of anesthesiology (11).
Future Directions
To date, anesthetic interventions focused on targeting acute pain have not demonstrated long-term functional benefits (12,13). Perhaps implementation of a PSH with better care coordination that includes individualized preoperative preparation and follow-up after surgery during rehabilitation will have greater potential for positive long-term outcomes. In addition to improvements in functional outcomes, a PSH may be able to provide patients a smoother transition from hospital to home in terms of pain management and decrease the incidence of chronic pain after common elective procedures like joint replacement (14). Finally, more health economic research is needed to prove the financial benefits of a PSH in terms of cost savings for hospitals.
In summary, the PSH is a model that can be applied many ways to provide coordinated care of the surgical patient from the decision to proceed with surgery through convalescence. Pain medicine plays an integral role in any PSH implementation. However, to be effective, anesthesiologists as leaders of the PSH need to target improvement strategies beyond pain outcomes and the immediate postoperative period.
The use of ultrasound guidance in the practice of regional anesthesia arguably began in the late 1980s (1), although ultrasound Doppler technology was used to direct needle insertion for peripheral nerve blockade in the 1970s (2). This past decade has seen a rapid increase in practical applications and clinical research in the field of ultrasound-guided regional anesthesia (UGRA), and the American Society of Regional Anesthesia and Pain Medicine (ASRA) and European Society of Regional Anesthesia have even published joint committee guidelines for training in this discipline (3).
Given the rapid adoption of UGRA, evidence to support this practice was initially limited; however, many studies have emerged in an attempt to define the role of ultrasound. In 2010, ASRA published a series of important articles which distill the body of evidence related to UGRA up to that time point (4-13). Additional studies have been completed and published since 2010 and will be included in an update that should be published in the next year.
Ultrasound Guidance for Extremity Peripheral Nerve Blocks
The 2010 ASRA systematic reviews covering this subject include 24 RCTs which compare ultrasound guidance to an alternative nerve localization technique for either upper or lower extremity peripheral nerve blockade (5). For both upper and lower extremity blocks, the majority of studies report faster block onset when ultrasound is employed (5,6,11), although 5 of 15 studies in the upper extremity and 2 of 5 studies in the lower extremity fail to find a difference in onset time (5). There is evidence to support a decrease in procedural time when ultrasound is used for upper and lower extremity blocks (6-11); however, set-up time and pre-scanning with ultrasound are not consistently measured or reported. In terms of block quality, lower extremity studies are more likely to report an advantage with ultrasound than upper extremity studies; only 4 of 16 upper extremity studies show improvement with ultrasound, and these studies use nerve stimulation or transarterial injection as the comparator (5). When a fixed time point is used for assessing block success, ultrasound use is more likely to show an advantage although the definitions of successful block vary widely (6,11). Only one study in the upper extremity shows a difference in block duration in favor of ultrasound while all other RCTs do not demonstrate a difference (5). For femoral and subgluteal sciatic nerve blocks, ultrasound use decreases the minimum effective anesthesia volume to achieve a successful block in 50% of patients (11).
Ultrasound for Continuous Peripheral Nerve Blocks
Although many large case series describing ultrasound-guided techniques for continuous peripheral nerve block (CPNB) performance have been published, there are relatively-fewer RCTs comparing ultrasound to other nerve localization techniques for CPNB. When an exclusively ultrasound-guided technique is compared to a stimulating catheter technique, procedural duration is shorter with ultrasound at four distinct insertion sites (14-17) with less procedure-related pain for lower extremity catheters (14,16) and fewer inadvertent vascular punctures for femoral and infraclavicular catheters (14,15). Most studies report similar analgesia and other acute pain outcomes from catheters placed with ultrasound when compared to other methods (18-20), with the exception of one study involving popliteal-sciatic catheters which suggests that stimulating catheters may provide an analgesic advantage although successful placement occurs less often (21).
Ultrasound for Truncal and Neuraxial Blocks
To date, RCTs comparing ultrasound guidance to traditional techniques for paravertebral blockade or transversus abdominis plane (TAP) blocks have yet to be reported. For both of these procedures, the 2010 ASRA systematic review recommends the use of ultrasound although this recommendation is based on case series data only (4). In one study comparing ultrasound-guided TAP to conventional ilioinguinal/iliohypogastric nerve blocks for inguinal hernia repair, subjects who received ultrasound-guided TAP blocks reported lower pain scores for the first 24 hours (22). Ultrasound-guidance and the landmark-based technique for ilioinguinal/iliohypogastric nerve blocks have been compared in children with the ultrasound-guided technique resulting in decreased need for systemic analgesic supplementation (23). For neuraxial blocks, there is evidence to support ultrasound scanning prior to employing conventional neuraxial block techniques rather than relying solely on surface landmarks (10), especially in patients with challenging anatomy (24).
Ultrasound for Regional Anesthesia in Special Populations
Ultrasound-guided techniques for peripheral (25) and neuraxial (26) blocks in children have been described previously. The 2010 ASRA evidence-based review on ultrasound for pediatric regional anesthesia included 6 RCTs involving peripheral nerve blocks and one randomized trial in neuraxial blockade in addition to case series of >10 patients (12). In this population, ultrasound may improve the speed of block onset and duration of analgesia, increase success rates for truncal blocks compared to blind techniques, and reduce the volume of local anesthetic required (12). In obese patients, ultrasound may play a role in identifying target peripheral and neuraxial structures as well as real-time procedural performance (27). When performing CPNB in obese patients, procedural time is not prolonged compared to non-obese patients when as long as ultrasound is used (28).
In summary, there is sufficient evidence to support the use of ultrasound guidance for peripheral nerve blockade based on short-term outcomes, and the results of a large prospective registry study suggest that ultrasound may decrease in the risk of local anesthetic systemic toxicity (29). Additional prospective studies are needed to further define the role of ultrasound in neuraxial blockade, long-term patient outcomes, and advantages in special populations.
References
Ting PL, Sivagnanaratnam V: Ultrasonographic study of the spread of local anaesthetic during axillary brachial plexus block. Br J Anaesth 1989; 63: 326-9
la Grange P, Foster PA, Pretorius LK: Application of the Doppler ultrasound bloodflow detector in supraclavicular brachial plexus block. Br J Anaesth 1978; 50: 965-7
Sites BD, Chan VW, Neal JM, Weller R, Grau T, Koscielniak-Nielsen ZJ, Ivani G: The American Society of Regional Anesthesia and Pain Medicine and the European Society Of Regional Anaesthesia and Pain Therapy Joint Committee recommendations for education and training in ultrasound-guided regional anesthesia. Reg Anesth Pain Med 2009; 34: 40-6
Abrahams MS, Horn JL, Noles LM, Aziz MF: Evidence-based medicine: ultrasound guidance for truncal blocks. Reg Anesth Pain Med 2010; 35: S36-42
Liu SS, Ngeow J, John RS: Evidence basis for ultrasound-guided block characteristics: onset, quality, and duration. Reg Anesth Pain Med 2010; 35: S26-35
McCartney CJ, Lin L, Shastri U: Evidence basis for the use of ultrasound for upper-extremity blocks. Reg Anesth Pain Med 2010; 35: S10-5
Narouze SN: Ultrasound-guided interventional procedures in pain management: Evidence-based medicine. Reg Anesth Pain Med 2010; 35: S55-8
Neal JM: Ultrasound-guided regional anesthesia and patient safety: An evidence-based analysis. Reg Anesth Pain Med 2010; 35: S59-67
Neal JM, Brull R, Chan VW, Grant SA, Horn JL, Liu SS, McCartney CJ, Narouze SN, Perlas A, Salinas FV, Sites BD, Tsui BC: The ASRA evidence-based medicine assessment of ultrasound-guided regional anesthesia and pain medicine: Executive summary. Reg Anesth Pain Med 2010; 35: S1-9
Perlas A: Evidence for the use of ultrasound in neuraxial blocks. Reg Anesth Pain Med 2010; 35: S43-6
Salinas FV: Ultrasound and review of evidence for lower extremity peripheral nerve blocks. Reg Anesth Pain Med 2010; 35: S16-25
Tsui BC, Pillay JJ: Evidence-based medicine: Assessment of ultrasound imaging for regional anesthesia in infants, children, and adolescents. Reg Anesth Pain Med 2010; 35: S47-54
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ: Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996; 17: 1-12
Mariano ER, Cheng GS, Choy LP, Loland VJ, Bellars RH, Sandhu NS, Bishop ML, Lee DK, Maldonado RC, Ilfeld BM: Electrical stimulation versus ultrasound guidance for popliteal-sciatic perineural catheter insertion: a randomized controlled trial. Reg Anesth Pain Med 2009; 34: 480-5
Mariano ER, Loland VJ, Bellars RH, Sandhu NS, Bishop ML, Abrams RA, Meunier MJ, Maldonado RC, Ferguson EJ, Ilfeld BM: Ultrasound guidance versus electrical stimulation for infraclavicular brachial plexus perineural catheter insertion. J Ultrasound Med 2009; 28: 1211-8
Mariano ER, Loland VJ, Sandhu NS, Bellars RH, Bishop ML, Afra R, Ball ST, Meyer RS, Maldonado RC, Ilfeld BM: Ultrasound guidance versus electrical stimulation for femoral perineural catheter insertion. J Ultrasound Med 2009; 28: 1453-60
Mariano ER, Loland VJ, Sandhu NS, Bellars RH, Bishop ML, Meunier MJ, Afra R, Ferguson EJ, Ilfeld BM: A trainee-based randomized comparison of stimulating interscalene perineural catheters with a new technique using ultrasound guidance alone. J Ultrasound Med 2010; 29: 329-336
Ilfeld BM: Continuous peripheral nerve blocks: a review of the published evidence. Anesth Analg 2011; 113: 904-25
Fredrickson MJ, Danesh-Clough TK: Ambulatory continuous femoral analgesia for major knee surgery: a randomised study of ultrasound-guided femoral catheter placement. Anaesth Intensive Care 2009; 37: 758-66
Choi S, Brull R: Is ultrasound guidance advantageous for interventional pain management? A review of acute pain outcomes. Anesth Analg 2011; 113: 596-604
Mariano ER, Loland VJ, Sandhu NS, Bishop ML, Lee DK, Schwartz AK, Girard PJ, Ferguson EJ, Ilfeld BM: Comparative efficacy of ultrasound-guided and stimulating popliteal-sciatic perineural catheters for postoperative analgesia. Can J Anaesth 2010; 57: 919-926
Aveline C, Le Hetet H, Le Roux A, Vautier P, Cognet F, Vinet E, Tison C, Bonnet F: Comparison between ultrasound-guided transversus abdominis plane and conventional ilioinguinal/iliohypogastric nerve blocks for day-case open inguinal hernia repair. Br J Anaesth 2011; 106: 380-6
Willschke H, Marhofer P, Bosenberg A, Johnston S, Wanzel O, Cox SG, Sitzwohl C, Kapral S: Ultrasonography for ilioinguinal/iliohypogastric nerve blocks in children. Br J Anaesth 2005; 95: 226-30
Chin KJ, Perlas A, Chan V, Brown-Shreves D, Koshkin A, Vaishnav V: Ultrasound imaging facilitates spinal anesthesia in adults with difficult surface anatomic landmarks. Anesthesiology 2011; 115: 94-101
Tsui B, Suresh S: Ultrasound imaging for regional anesthesia in infants, children, and adolescents: a review of current literature and its application in the practice of extremity and trunk blocks. Anesthesiology 2010; 112: 473-92
Tsui BC, Suresh S: Ultrasound imaging for regional anesthesia in infants, children, and adolescents: a review of current literature and its application in the practice of neuraxial blocks. Anesthesiology 2010; 112: 719-28
Brodsky JB, Mariano ER: Regional anaesthesia in the obese patient: lost landmarks and evolving ultrasound guidance. Best Pract Res Clin Anaesthesiol 2011; 25: 61-72
Mariano ER, Brodsky JB: Comparison of procedural times for ultrasound-guided perineural catheter insertion in obese and nonobese patients. J Ultrasound Med 2011; 30: 1357-61
Barrington MJ, Kluger R: Ultrasound guidance reduces the risk of local anesthetic systemic toxicity following peripheral nerve blockade. Reg Anesth Pain Med 2013; 38: 289-297
I wear a lot of hats in my job. Though I’m a physician who specializes in the practice of anesthesiology, I don’t spend all day every day at the head of an operating room table.
Many days I spend in an administrative leadership role or conducting research studies. These functions support the best interests of my patients as well as the science and practice of anesthesiology. On my “clinical” days that I spend in hands-on patient care, I provide anesthesia for patients who undergo surgery and other invasive procedures. I also treat acute pain as a consultant. Some of my colleagues in anesthesiology specialize in chronic pain or critical care medicine.
As a medical student, I had a hard time at first understanding what the physician anesthesiologist does. I saw monitors, complicated equipment, and technical procedures that involved a lot of needles. Thankfully, I worked with resident and attending anesthesiologists who inspired me to pursue this specialty.
Anesthesiology is a unique field within medicine. It is at the same time incredibly cerebral and extremely physical. For example, the physician anesthesiologist must be ready to diagnose heart or lung problems that may complicate the patient’s surgery, and decide which medications are appropriate.
Before administering a medication, it’s not enough just to understand the complex pharmacologic effects of the drug and determine the right dose. The anesthesiologist also has to know how to dilute and prepare the drug, the appropriate route for the medication, which other medications are and are not compatible, and how to program the infusion device. In addition, an anesthesiologist has to be technically skilled at finding veins—sometimes in the hand or arm, sometimes leading centrally to the heart—in order to give the medication in the first place.
I am always aware of the trust that patients and their families give me, a total stranger, and I work hard to earn that trust throughout the perioperative period. The job of the physician anesthesiologist is deeply personal. In the operating room, I care for the most vulnerable of patients—those who, while under anesthesia, cannot care for themselves.
– I constantly listen to the sounds of their hearts. – I breathe for them when they are unable. – I keep them warm in the cold operating room. – I provide the fluids that their bodies need. – I pad their arms and legs and other pressure points. – I watch the operation step by step, anticipating and responding. – I learn from their bodies’ response to anesthesia to give the right amount. – I prevent and relieve their pain. – I protect them from dangers of which they are unaware.
I have heard people, my colleagues included, compare physician anesthesiologists to pilots. No one claps when the plane lands, just as no one expects any less than a perfect uncomplicated anesthetic every time. We physician anesthesiologists draw great personal satisfaction from doing what we do, and from providing a unique type of personalized medicine. Our patients and their families depend on us to be at our best, always.
The concept of preoperative preparation for patients scheduled for surgery requiring anesthesia is not a new one. In fact, the idea goes back to Dr. Albert Lee’s description in 1949 (1, 2). Dr. Lee had observed in his day that patients commonly presented for surgery in various states of poor health; it seemed to make more sense to see these patients before surgery to identify areas of concern early and optimize patients’ conditions they went under the knife.
The model of a stand-alone preoperative evaluation clinic, often run by anesthesiology staff, with a “one stop shop” model for patients’ interviews and examinations, testing, education, and referrals really did not take off until the 1990s (3). This patient-centered care model was intended to improve efficiency by decreasing the run-around that many patients encountered, but it also saved money for the institution by reducing the ordering of unnecessary tests (4) and decreasing day-of-surgery cancellations (4, 5).
Current State
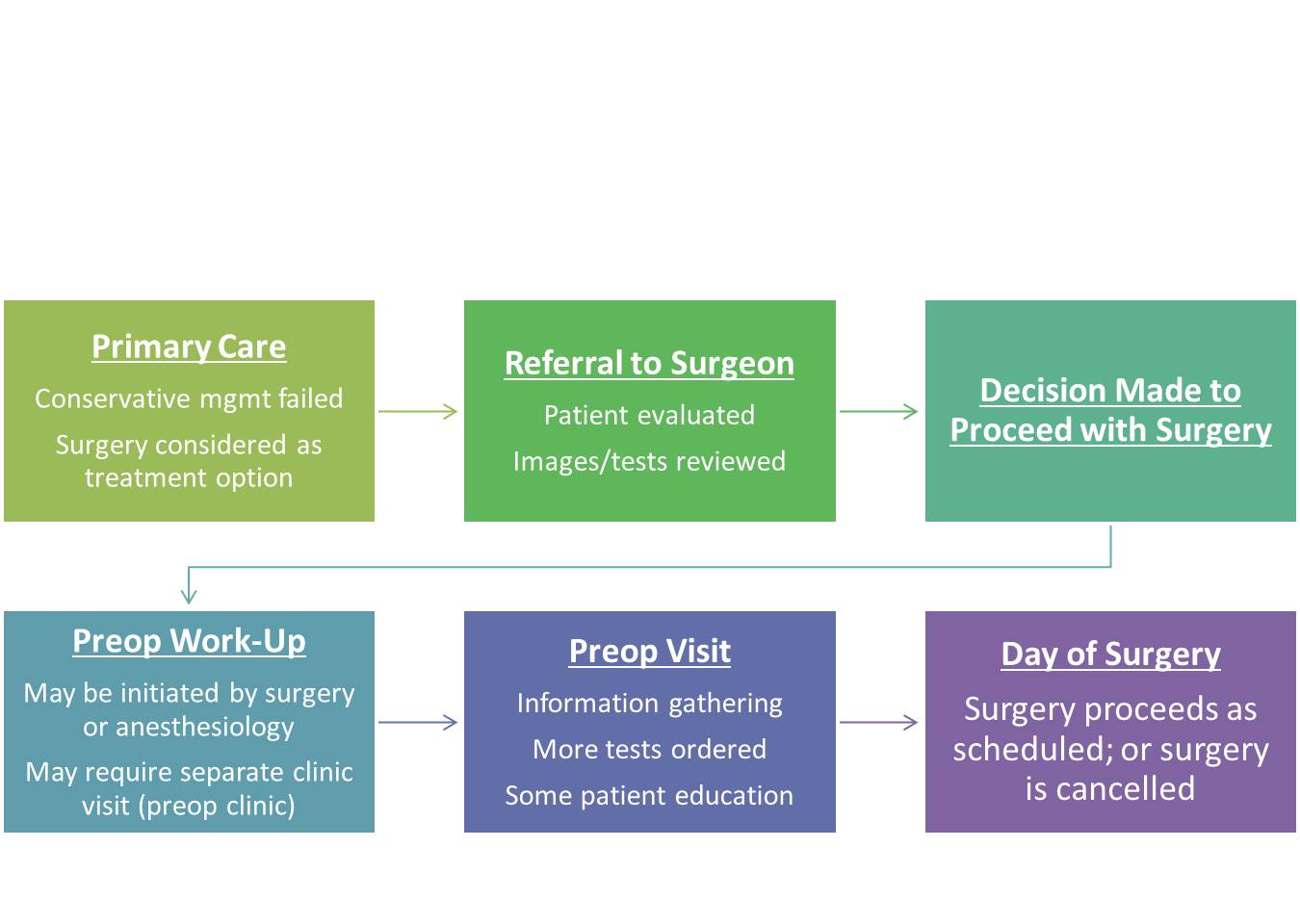
In the present state (assuming an ACO or HMO model), patients are referred to the surgeon by the primary care physician for evaluation of a problem that may be amenable to surgical correction. If the surgeon deems the patient a surgical candidate, the patient may receive a scheduled date for surgery and then may be referred to the anesthesiology preoperative evaluation clinic (“preop clinic”) for further work-up. During this encounter, the provider in the preop clinic may request a variety of tests based on the planned surgery and the patient’s comorbid conditions in order to make appropriate recommendations regarding perioperative management to minimize risks. The American Society of Anesthesiologists (ASA) has published a recent (2012) practice advisory for preanesthesia evaluation to guide this process.
Unfortunately, after nearly 2 decades of employing this model, day of surgery cancellations still occur at various rates around the world. Some of the reasons are related to factors that preop clinics were meant to avoid: inadequate preoperative work-up or change in medical condition (6). Other reasons are patient-driven: patients’ not showing up (7) or patients’ changing their minds about having surgery (8). Although not all of these issues are easily solved, it does make me wonder–perhaps it is time for us to rethink the process of preparing patients for surgery.
In our current state, a patient may hypothetically be scheduled for surgery in 8 weeks, a date agreed upon by the patient and surgeon based on available dates. Even if a preop clinic visit takes place the same day as the surgery clinic visit, this only allows 2 months to optimize a patient’s chronic medical conditions (e.g., hypertension, diabetes, coronary artery disease) that took years to develop. Imagine if the timeline was even shorter, like 3 weeks. Add to this time pressure the tremendous physiologic stress that surgery and the subsequent rehabilitation put on the body, and it is not difficult to see why patients can still be cancelled on the day of surgery when they present with abnormal vital signs or test results, making the risks seem too high. We would not expect ourselves to run a marathon without adequate training and preparation on short notice–why would we do this to our patients having elective surgery?
Future State
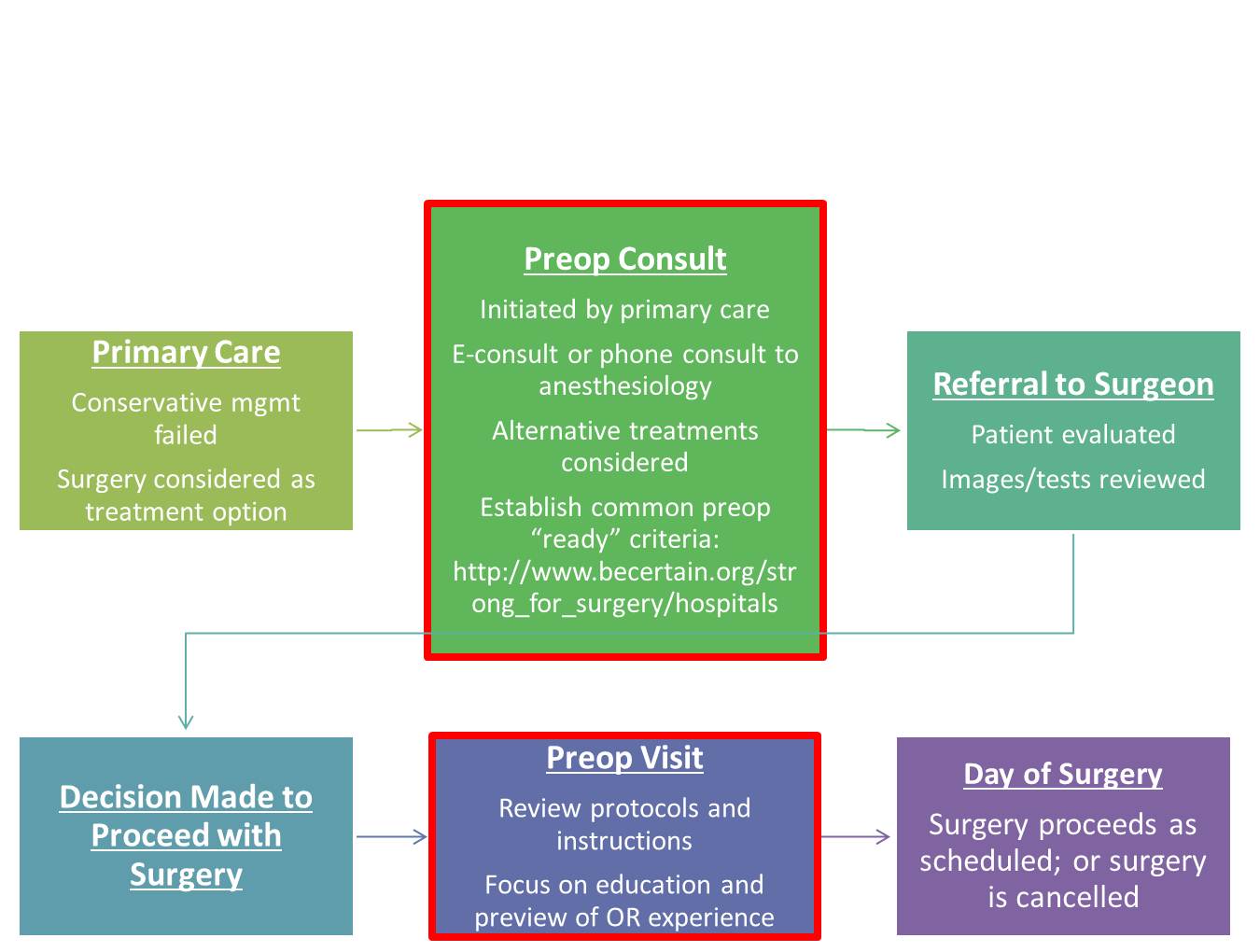
How can we improve preoperative preparation? I think it still starts with the primary care physician. With advances in technology such as telemedicine and e-consults (or low-tech phone calls), we have ways to create a direct interface between primary care physicians and anesthesiologists to discuss advanced preparation of patients who may undergo elective surgical procedures.
This coordinated care model is consistent with ASA’s Perioperative Surgical Home. Early consultation may involve assessment of a patient’s risks and benefits from the procedure, consideration of alternative treatments, and development of a plan to optimize the patient’s comorbid conditions, medication management, and nutrition. Strong for Surgery is a program that provides patients and clinicians useful checklists based on best-available evidence to guide early preoperative preparation related to smoking cessation, nutrition, glycemic control, and medication management. For elective surgery, the decision when to refer the patient to a surgeon can be made jointly by the primary care physician and anesthesiologist. Prior to surgery, the preop clinic visit should still take place, but the focus no longer needs to be on information-gathering and ordering a battery of tests; rather, the goals should be to review pertinent instructions, preview the perioperative experience for patients, and address any logistical or scheduling issues raised by patients to prevent their not showing up or changing their minds at the last minute. Let’s get started.
Among Medicare beneficiaries in the United States, the number of primary total knee arthroplasty (TKA) procedures from 1991 to 2010 increased by 161.5% (1). Postoperative pain remains one of patients’ top concerns when undergoing elective surgery (2) and can limit patients’ functional ability in the early postoperative period (3). Providing effective perioperative pain control has potential longer-term implications since early rehabilitation may lead to improvements in functional outcomes later on (4). With the ability to select specific targets for local anesthetic injection and infusion, regional anesthesia techniques, neuraxial and peripheral, are commonly included in the perioperative analgesic protocol for joint arthroplasty patients (5-11). While the data supporting the analgesic efficacy of regional anesthesia techniques in this setting are strongly positive, studies attempting to attribute functional outcome benefits to regional anesthesia demonstrate mixed results.
The main challenge in assessing functional outcomes following joint replacement is the selection of outcomes; these can be divided into performance-based outcomes and self-reported outcomes (12, 13). Performance-based outcomes are measurable and arguably more objective, although often subject to effort. Examples of these outcomes and their units of measure include joint range of motion in degrees (e.g., flexion, extension, rotation); timed walking tests in meters (e.g., 6 minute walking test [6MWT], 2 minute walking test [2MWT]); muscle strength in units of force using a dynamometer (e.g., maximum voluntary isometric contraction [MVIC]); and timed up-and-go (TUG) in minutes (12, 13). Self-reported outcomes are typically survey-based; examples include the Western Ontario McMaster Universities Osteoarthritis Index (WOMAC), Knee Society Score, and Lower Extremity Functional Scale (12, 13). Since patient perception of successful rehabilitation is an important factor, self-reported outcomes should be reported with performance-based outcomes (12). Another important challenge when measuring and comparing functional outcomes is that clinical pathways for joint arthroplasty that integrate pain management (including regional analgesia), physical therapy, nursing, and surgical care are often specific to individual institutions, and institutions may vary with respect to rehabilitation goals and the timeline to achieve them.
Epidural Analgesia
Epidural analgesia has been used for perioperative pain management in joint replacement patients since at least the 1980s (14, 15). In 1987, Raj and colleagues compared postoperative systemic opioid analgesia to continuous epidural analgesia (bupivacaine 0.25% at 6-15 ml/hr) for TKA patients in a prospective non-randomized study (14). Although pain scores were lower in the epidural group, not surprisingly a high proportion of these patients experienced complete motor block of the lower extremities; although the authors mention “rigorous passive exercises,” specific rehabilitation outcomes were not reported (14). Later studies have reported functional benefits associated with continuous epidural analgesia, such as shorter time to achieve ambulation distance and range of motion goals, when compared to parenteral opioids alone (16). At institutions where continuous epidural analgesia is currently employed as part of a multimodal analgesic protocol, very low doses of local anesthetic (e.g., 0.06% bupivacaine) in combination with opioid are used in order to minimize motor block (17).
Peripheral Nerve Blocks
The innervation of the knee is complex and involves contributions from both the lumbar and sacral plexuses. While epidural analgesia is effective, it is also associated with clinically-significant side effects (e.g., nausea/vomiting and motor block of the non-operative limb) (5, 18) and the potential for neuraxial hematoma in patients on pharmacologic thromboprophylaxis (19). Thus, peripheral nerve block options, either single-injection or continuous infusions, have been explored for postoperative pain management.
Two early studies by Capdevila (6) and Singelyn (20) have shown continuous femoral nerve block (FNB) to provide comparable analgesia and physical therapy outcome achievement with fewer side effects when compared to epidural analgesia. Both of these studies also demonstrated shorter hospital length of stay for the regional anesthesia groups compared to an opioid-only group (6, 20), but hospitalization duration for these studies was, on average, greater than what has been reported in other studies (21). Triple-masked, placebo-controlled randomized clinical trials have shown that CPNB can shorten the time to achieve discharge criteria, including 100 m ambulation distance, for TKA (10, 22) and total hip arthroplasty (THA) (9) patients, but actual hospital duration was similar in these studies.
One of the interesting findings from the Singelyn study was that regional anesthesia patients maintained a knee flexion advantage over the opioid-only group at 6 week follow-up (20); although this advantage did not remain at 3 months, this finding supported the potential for long-term functional improvement resulting from effective pain management and early rehabilitation in the immediate perioperative period (4). In a randomized comparison of continuous FNB to local infiltration analgesia (LIA) for TKA, the FNB group spent more time out of bed walking; at 6 weeks, the FNB group showed more improvement in performance-based (6MWT) and self-reported functional outcome assessments (23). In contrast, the one year follow-up studies of randomized clinical trial subjects (9, 10, 22) using self-reported outcome measures for functional status (WOMAC) did not show long-term improvement associated with regional anesthesia techniques (24-27).
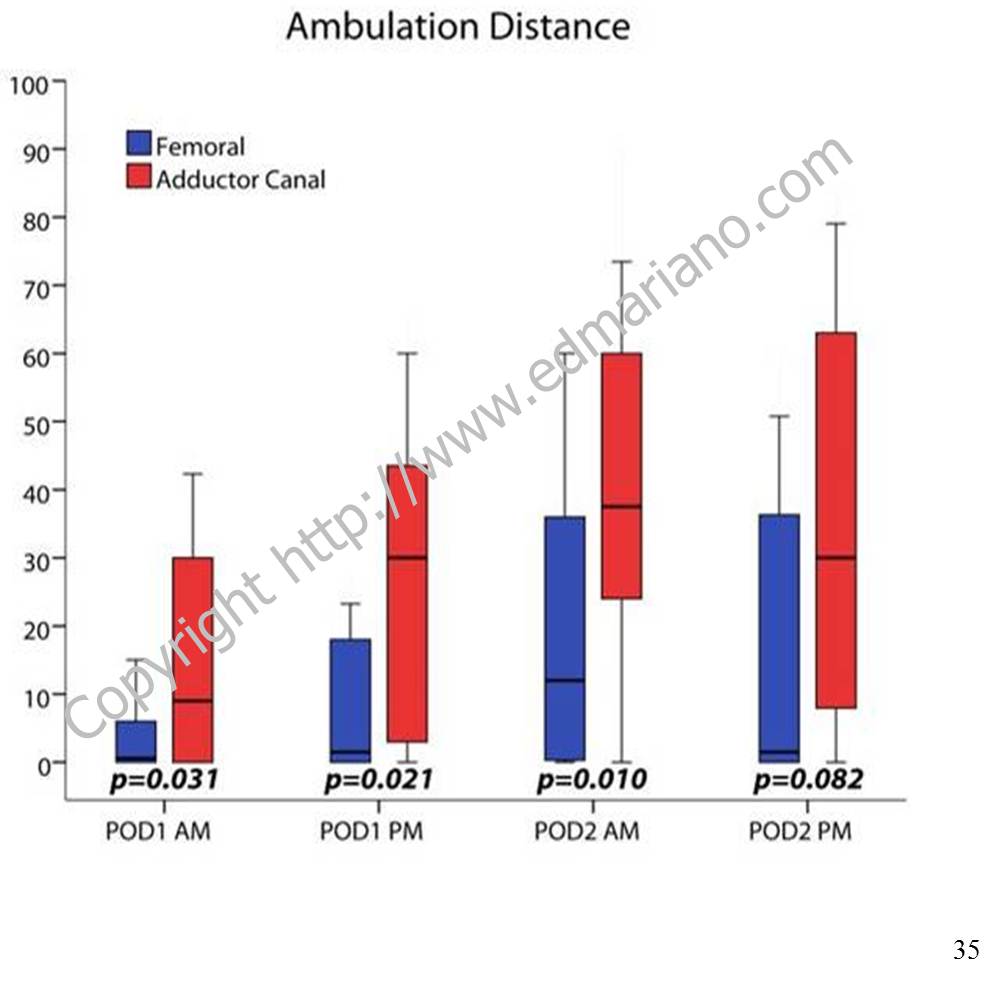
The rehabilitation outcome measured in the immediate postoperative period that correlates best with long-term functional improvement is not yet established. Ambulation distance is often measured by physical therapists and included in discharge criteria (9, 10, 22). For institutions that emphasize ambulation in their clinical pathway for lower extremity joint arthroplasty, a major concern raised with regard to FNBs is the potential association with increased fall risk (28, 29) although a recent large database study disputes this finding. In-hospital falls can lead to prolonged hospital stays with higher costs and are associated with more frequent postoperative complications, including serious organ system dysfunction and death (30). With currently-available local anesthetic solutions and typical doses, perineural infusion does produce clinically-significant quadriceps weakness when administered near the femoral nerve or lumbar plexus (31, 32). Since the local anesthetics themselves cannot select sensory over motor nerves( 33), anesthesiologists have started exploring alternate nerve block locations to minimize the risk of motor block and maximize patient rehabilitation.
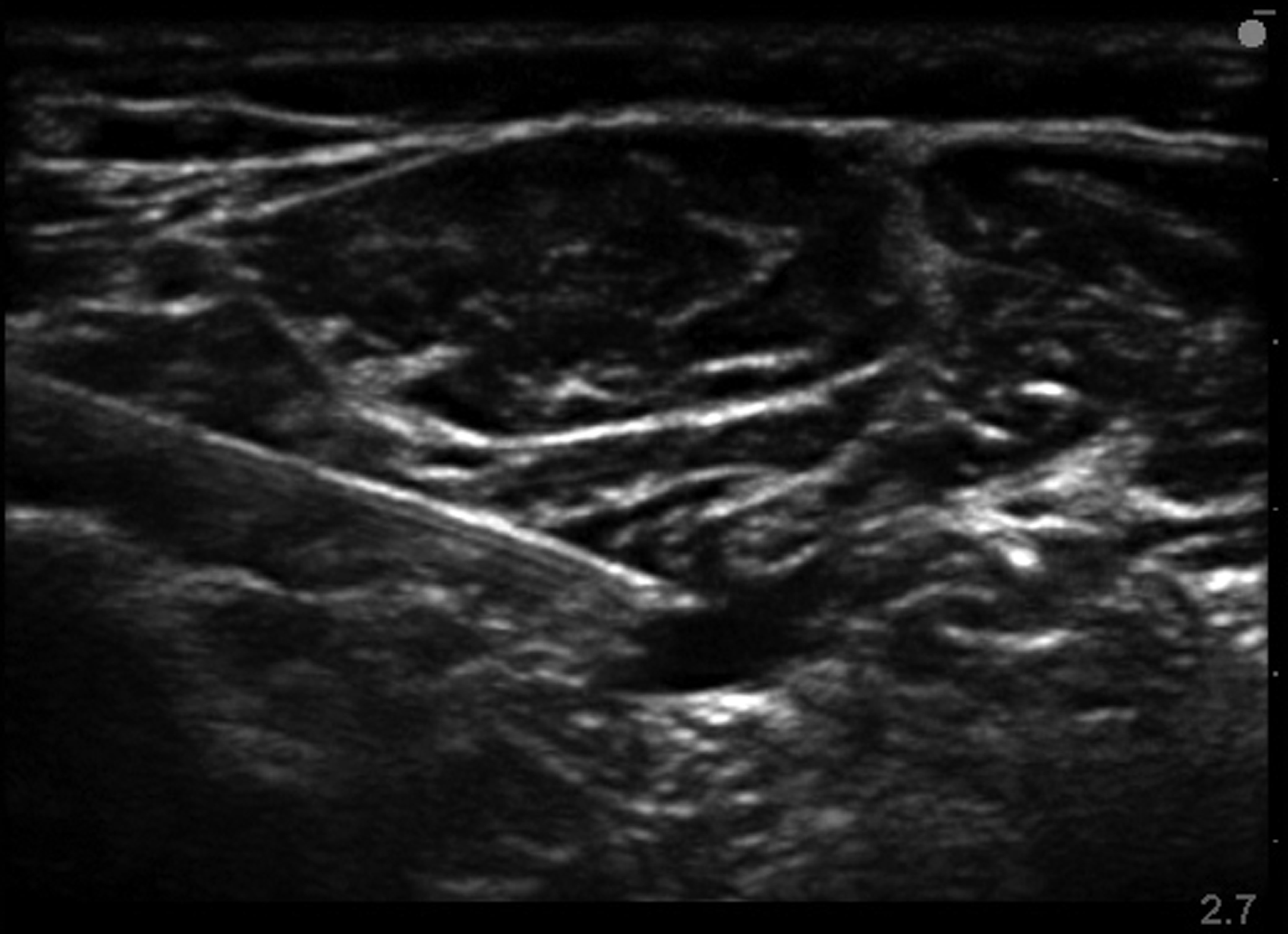
From Workman JJ, et al. Presented at 2013 ASRA Spring Annual Meeting
For TKA, a more distal nerve block location in the adductor canal can provide effective analgesia postoperatively (34) and has been shown to better preserve quadriceps strength compared to a FNB in both volunteers (35) and clinical patients (11). Regional analgesic techniques are only one part of the overall pain management plan. While they are often included in multimodal analgesic protocols along with non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and low-dose opioids (36), there is a growing body of evidence to support the adductor canal block as the regional analgesic technique of choice for promoting postoperative ambulation within a clinical pathway (37, 38).
For patient information with answers to frequently-asked questions about regional anesthesia, please see “Regional Anesthesia FAQs.”
References
Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991-2010. JAMA. Sep 26 2012;308(12):1227-1236.
Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg. Sep 1999;89(3):652-658.
Holm B, Kristensen MT, Myhrmann L, et al. The role of pain for early rehabilitation in fast track total knee arthroplasty. Disability and rehabilitation. 2010;32(4):300-306.
Munin MC, Rudy TE, Glynn NW, Crossett LS, Rubash HE. Early inpatient rehabilitation after elective hip and knee arthroplasty. JAMA. Mar 18 1998;279(11):847-852.
Barrington MJ, Olive D, Low K, Scott DA, Brittain J, Choong P. Continuous femoral nerve blockade or epidural analgesia after total knee replacement: a prospective randomized controlled trial. Anesth Analg. Dec 2005;101(6):1824-1829.
Capdevila X, Barthelet Y, Biboulet P, Ryckwaert Y, Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology. Jul 1999;91(1):8-15.
Chelly JE, Greger J, Gebhard R, et al. Continuous femoral blocks improve recovery and outcome of patients undergoing total knee arthroplasty. J Arthroplasty. Jun 2001;16(4):436-445.
Hebl JR, Dilger JA, Byer DE, et al. A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. Reg Anesth Pain Med. Nov-Dec 2008;33(6):510-517.
Ilfeld BM, Ball ST, Gearen PF, et al. Ambulatory continuous posterior lumbar plexus nerve blocks after hip arthroplasty: a dual-center, randomized, triple-masked, placebo-controlled trial. Anesthesiology. Sep 2008;109(3):491-501.
Ilfeld BM, Le LT, Meyer RS, et al. Ambulatory continuous femoral nerve blocks decrease time to discharge readiness after tricompartment total knee arthroplasty: a randomized, triple-masked, placebo-controlled study. Anesthesiology. Apr 2008;108(4):703-713.
Jaeger P, Zaric D, Fomsgaard JS, et al. Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: a randomized, double-blind study. Reg Anesth Pain Med. Nov-Dec 2013;38(6):526-532.
Choi S, Trang A, McCartney CJ. Reporting functional outcome after knee arthroplasty and regional anesthesia: a methodological primer. Reg Anesth Pain Med. Jul-Aug 2013;38(4):340-349.
Bernucci F, Carli F. Functional outcome after major orthopedic surgery: the role of regional anesthesia redefined. Curr Opin Anaesthesiol. Oct 2012;25(5):621-628.
Raj PP, Knarr DC, Vigdorth E, et al. Comparison of continuous epidural infusion of a local anesthetic and administration of systemic narcotics in the management of pain after total knee replacement surgery. Anesth Analg. May 1987;66(5):401-406.
Pettine KA, Wedel DJ, Cabanela ME, Weeks JL. The use of epidural bupivacaine following total knee arthroplasty. Orthopaedic review. Aug 1989;18(8):894-901.
Mahoney OM, Noble PC, Davidson J, Tullos HS. The effect of continuous epidural analgesia on postoperative pain, rehabilitation, and duration of hospitalization in total knee arthroplasty. Clin Orthop Relat Res. Nov 1990(260):30-37.
YaDeau JT, Cahill JB, Zawadsky MW, et al. The effects of femoral nerve blockade in conjunction with epidural analgesia after total knee arthroplasty. Anesth Analg. Sep 2005;101(3):891-895, table of contents.
Zaric D, Boysen K, Christiansen C, Christiansen J, Stephensen S, Christensen B. A comparison of epidural analgesia with combined continuous femoral-sciatic nerve blocks after total knee replacement. Anesth Analg. Apr 2006;102(4):1240-1246.
Horlocker TT, Wedel DJ, Rowlingson JC, et al. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Reg Anesth Pain Med. Jan-Feb 2010;35(1):64-101.
Singelyn FJ, Deyaert M, Joris D, Pendeville E, Gouverneur JM. Effects of intravenous patient-controlled analgesia with morphine, continuous epidural analgesia, and continuous three-in-one block on postoperative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg. Jul 1998;87(1):88-92.
Salinas FV, Liu SS, Mulroy MF. The effect of single-injection femoral nerve block versus continuous femoral nerve block after total knee arthroplasty on hospital length of stay and long-term functional recovery within an established clinical pathway. Anesth Analg. Apr 2006;102(4):1234-1239.
Ilfeld BM, Mariano ER, Girard PJ, et al. A multicenter, randomized, triple-masked, placebo-controlled trial of the effect of ambulatory continuous femoral nerve blocks on discharge-readiness following total knee arthroplasty in patients on general orthopaedic wards. Pain. Sep 2010;150(3):477-484.
Carli F, Clemente A, Asenjo JF, et al. Analgesia and functional outcome after total knee arthroplasty: periarticular infiltration vs continuous femoral nerve block. Br J Anaesth. Aug 2010;105(2):185-195.
Ilfeld BM, Shuster JJ, Theriaque DW, et al. Long-term pain, stiffness, and functional disability after total knee arthroplasty with and without an extended ambulatory continuous femoral nerve block: a prospective, 1-year follow-up of a multicenter, randomized, triple-masked, placebo-controlled trial. Reg Anesth Pain Med. Mar-Apr 2011;36(2):116-120.
Morin AM, Kratz CD, Eberhart LH, et al. Postoperative analgesia and functional recovery after total-knee replacement: comparison of a continuous posterior lumbar plexus (psoas compartment) block, a continuous femoral nerve block, and the combination of a continuous femoral and sciatic nerve block. Reg Anesth Pain Med. Sep-Oct 2005;30(5):434-445.
Ilfeld BM, Ball ST, Gearen PF, et al. Health-related quality of life after hip arthroplasty with and without an extended-duration continuous posterior lumbar plexus nerve block: a prospective, 1-year follow-up of a randomized, triple-masked, placebo-controlled study. Anesth Analg. Aug 2009;109(2):586-591.
Ilfeld BM, Meyer RS, Le LT, et al. Health-related quality of life after tricompartment knee arthroplasty with and without an extended-duration continuous femoral nerve block: a prospective, 1-year follow-up of a randomized, triple-masked, placebo-controlled study. Anesth Analg. Apr 2009;108(4):1320-1325.
Feibel RJ, Dervin GF, Kim PR, Beaule PE. Major complications associated with femoral nerve catheters for knee arthroplasty: a word of caution. J Arthroplasty. Sep 2009;24(6 Suppl):132-137.
Ilfeld BM, Duke KB, Donohue MC. The association between lower extremity continuous peripheral nerve blocks and patient falls after knee and hip arthroplasty. Anesth Analg. Dec 2010;111(6):1552-1554.
Memtsoudis SG, Dy CJ, Ma Y, Chiu YL, Della Valle AG, Mazumdar M. In-hospital patient falls after total joint arthroplasty: incidence, demographics, and risk factors in the United States. J Arthroplasty. Jun 2012;27(6):823-828 e821.
Charous MT, Madison SJ, Suresh PJ, et al. Continuous femoral nerve blocks: varying local anesthetic delivery method (bolus versus basal) to minimize quadriceps motor block while maintaining sensory block. Anesthesiology. Oct 2011;115(4):774-781.
Ilfeld BM, Moeller LK, Mariano ER, et al. Continuous peripheral nerve blocks: is local anesthetic dose the only factor, or do concentration and volume influence infusion effects as well? Anesthesiology. Feb 2010;112(2):347-354.
Ilfeld BM, Yaksh TL. The end of postoperative pain–a fast-approaching possibility? And, if so, will we be ready? Reg Anesth Pain Med. Mar-Apr 2009;34(2):85-87.
Lund J, Jenstrup MT, Jaeger P, Sorensen AM, Dahl JB. Continuous adductor-canal-blockade for adjuvant post-operative analgesia after major knee surgery: preliminary results. Acta Anaesthesiol Scand. Jan 2011;55(1):14-19.
Jaeger P, Nielsen ZJ, Henningsen MH, Hilsted KL, Mathiesen O, Dahl JB. Adductor Canal Block versus Femoral Nerve Block and Quadriceps Strength: A Randomized, Double-blind, Placebo-controlled, Crossover Study in Healthy Volunteers. Anesthesiology. Feb 2013;118(2):409-415.
Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. Feb 2012;116(2):248-273.
Perlas A, Kirkham KR, Billing R, et al. The impact of analgesic modality on early ambulation following total knee arthroplasty. Reg Anesth Pain Med. Jul-Aug 2013;38(4):334-339.
Mudumbai SC, Kim TE, Howard SK, et al. Continuous adductor canal blocks are superior to continuous femoral nerve blocks in promoting early ambulation after TKA. Clin Orthop Relat Res. 2014 May;472(5):1377-83.
Since 2012, the American Society of Anesthesiologists has promoted the Perioperative Surgical Home model in which anesthesiologists function as leaders in the coordination of perioperative care for surgical patients to improve outcomes (1,2). While anesthesiologists globally have had similar interests over the years, the unifying challenge continues to be the selection of outcomes and demonstration of improvement due to the anesthesiologist’s role and/or choice of anesthetic or analgesic technique. Since the types of outcomes and frequency of occurrence vary widely, a comprehensive discussion of perioperative outcomes is beyond the scope of this summary. Therefore, this review will focus on select anesthesiologist-driven factors related to acute pain management and anesthetic technique on perioperative outcomes and potential research directions.
Rare Outcomes and Big Data
For anesthesiologists, avoiding adverse events of the lowest frequency (death, recall, and nerve injury) receives highest priority with death ranking first among complications to avoid (3). Studies involving rare outcomes, positive or negative, will invariably require accumulation of “big data.” Such studies must either involve multiple institutions over a long study period (if prospective) or access data involving a large cohort of patients for retrospective studies; these study designs involving longitudinal data may also require advanced statistical methods (4). For example, Memtsoudis and colleagues sought to evaluate postoperative morbidity and mortality for lower extremity joint arthroplasty patients in a recent study (5). They utilized a large nationwide administrative database maintained by Premier Perspective, Inc. (Charlotte, NC, USA); the study data were gathered from 382,236 patients in approximately 400 acute care hospitals throughout the United States over 4 years (5). Other retrospective cohort studies comparing the occurrence of perioperative complications such as surgical site infections, cardiopulmonary morbidity, and mortality have used the American College of Surgeons National Surgical Quality Improvement Project (NSQIP) (6-8). NSQIP originally started within the Veterans Health Administration (VHA) system in the 1980s with a small sample of hospitals; this project, which included public reporting of outcomes data, eventually expanded to include all VHA surgical facilities and others outside the VHA system (9). Multi-center prospective registries such as the SOS Regional Anesthesia Hotline (10, 11) and AURORA (12, 13) have been developed for outcomes research and have reported the occurrence rates of rare complications related to regional anesthesia. The disadvantages to these data-driven studies include lack or randomization introducing potential bias, missing or incorrectly coded data, inability to draw conclusions regarding causation, and restrictions to access such as information security issues and/or cost (e.g., the Premier database). However, these retrospective cohort database studies may offer large samples sizes and administrative data from actual “real world” patients over a longer period of time and may identify important associations that influence clinical practice and generate hypotheses for future prospective studies.
Anesthesia Type and Perioperative Mortality
Based on the study by Memtsoudis and colleagues, overall 30-day mortality for lower extremity arthroplasty patients is lower for patients who receive neuraxial and combined neuraxial-general anesthesia compared to general anesthesia alone (5). In most categories, the rates of occurrence of in-hospital complications are also lower for the neuraxial and combined neuraxial-general anesthesia groups vs. the general anesthesia group, and transfusion requirements are lowest for the neuraxial group compared to all other groups (5). Studies using NSQIP have reported no difference in 30-day mortality for carotid endarterectomy patients associated with anesthetic technique although regional anesthesia patients are more likely to have a shorter operative time and next-day discharge (8); similarly, there is no difference in 30-day mortality for endovascular aortic aneurysm repair although general anesthesia patients are more likely to have longer length of stay and pulmonary complications (14).
Perioperative Analgesia and Cancer Recurrence
In a relatively-small matched retrospective study, Exadaktylos and colleagues have reported lower rates of recurrence and metastasis for breast cancer surgery patients who receive paravertebral analgesia vs. conventional systemic opioids (15). Although the exact mechanism was not well-understood at that time (regional anesthesia vs. reduction in the use of anesthetic agents and opioids), clinical and basic science research in this area has grown rapidly and has demonstrated mixed results. A follow-up study involving 503 patients who underwent abdominal surgery for cancer and were previously enrolled in a large multi-center clinical trial (16) and a retrospective database study of 424 colorectal cancer patients who underwent laparoscopic resection (17) have not shown a difference in recurrence-free survival or mortality. A recent meta-analysis including 14 prospective and retrospective studies involving cancer patients (colorectal, ovarian, breast, prostate, and hepatocellular) demonstrates a positive association between epidural analgesia and overall survival but no difference in recurrence-free survival compared to general anesthesia with opioid analgesia (18).
Analgesic Technique and Persistent Postsurgical Pain
Chronic pain may develop after many common operations including breast surgery, hernia repair, thoracic surgery, and amputation and is associated with severe acute pain in the postoperative period (19). While regional analgesic techniques are effective for acute pain management, currently-available data are inconclusive with regard to their ability to prevent the development of persistent postsurgical pain (20-22). There is an opportunity to use larger databases to investigate this issue further.
Ultrasound and Patient Safety
In 2010, the American Society of Regional Anesthesia and Pain Medicine published a series of articles presenting the evidence basis for ultrasound in regional anesthesia (23). According to the article focused on patient safety, evidence at the time suggested that ultrasound may decrease the incidence of minor adverse events (e.g., hemidiaphragmatic paresis from interscalene block or inadvertent vascular puncture), but serious complications such as local anesthetic systemic toxicity (LAST) and nerve injury did not occur at different rates based on the nerve localization technique (24). Since then, a large prospective multi-center registry study has shown that the use of ultrasound in regional anesthesia does reduce the incidence of LAST compared to traditional techniques (13). Similar methodology may be applied to other rare complications associated with anesthetic interventions.
Perioperative Medicine and Health Care Costs
Approximately 31% of costs related to inpatient perioperative care is attributable to the ward admission (25). Anesthesiologists as perioperative physicians have an opportunity to influence the cost of surgical care by decreasing hospital length of stay through effective pain management and by developing coordinated multi-disciplinary clinical pathways (26, 27).
REFERENCES
Vetter TR, Goeddel LA, Boudreaux AM, Hunt TR, Jones KA, Pittet JF. The Perioperative Surgical Home: how can it make the case so everyone wins? BMC anesthesiology. 2013;13:6.
Vetter TR, Ivankova NV, Goeddel LA, McGwin G, Jr., Pittet JF. An Analysis of Methodologies That Can Be Used to Validate if a Perioperative Surgical Home Improves the Patient-centeredness, Evidence-based Practice, Quality, Safety, and Value of Patient Care. Anesthesiology. Dec 2013;119(6):1261-1274.
Macario A, Weinger M, Truong P, Lee M. Which clinical anesthesia outcomes are both common and important to avoid? The perspective of a panel of expert anesthesiologists. Anesth Analg. May 1999;88(5):1085-1091.
Ma Y, Mazumdar M, Memtsoudis SG. Beyond repeated-measures analysis of variance: advanced statistical methods for the analysis of longitudinal data in anesthesia research. Reg Anesth Pain Med. Jan-Feb 2012;37(1):99-105.
Memtsoudis SG, Sun X, Chiu YL, et al. Perioperative comparative effectiveness of anesthetic technique in orthopedic patients. Anesthesiology. May 2013;118(5):1046-1058.
Liu J, Ma C, Elkassabany N, Fleisher LA, Neuman MD. Neuraxial anesthesia decreases postoperative systemic infection risk compared with general anesthesia in knee arthroplasty. Anesth Analg. Oct 2013;117(4):1010-1016.
Radcliff TA, Henderson WG, Stoner TJ, Khuri SF, Dohm M, Hutt E. Patient risk factors, operative care, and outcomes among older community-dwelling male veterans with hip fracture. J Bone Joint Surg Am. Jan 2008;90(1):34-42.
Schechter MA, Shortell CK, Scarborough JE. Regional versus general anesthesia for carotid endarterectomy: the American College of Surgeons National Surgical Quality Improvement Program perspective. Surgery. Sep 2012;152(3):309-314.
Ingraham AM, Richards KE, Hall BL, Ko CY. Quality improvement in surgery: the American College of Surgeons National Surgical Quality Improvement Program approach. Advances in surgery. 2010;44:251-267.
Auroy Y, Benhamou D, Bargues L, et al. Major complications of regional anesthesia in France: The SOS Regional Anesthesia Hotline Service. Anesthesiology. Nov 2002;97(5):1274-1280.
Auroy Y, Narchi P, Messiah A, Litt L, Rouvier B, Samii K. Serious complications related to regional anesthesia: results of a prospective survey in France. Anesthesiology. Sep 1997;87(3):479-486.
Barrington MJ, Watts SA, Gledhill SR, et al. Preliminary results of the Australasian Regional Anaesthesia Collaboration: a prospective audit of more than 7000 peripheral nerve and plexus blocks for neurologic and other complications. Reg Anesth Pain Med. Nov-Dec 2009;34(6):534-541.
Barrington MJ, Kluger R. Ultrasound guidance reduces the risk of local anesthetic systemic toxicity following peripheral nerve blockade. Reg Anesth Pain Med. Jul-Aug 2013;38(4):289-297.
Edwards MS, Andrews JS, Edwards AF, et al. Results of endovascular aortic aneurysm repair with general, regional, and local/monitored anesthesia care in the American College of Surgeons National Surgical Quality Improvement Program database. J Vasc Surg. Nov 2011;54(5):1273-1282.
Exadaktylos AK, Buggy DJ, Moriarty DC, Mascha E, Sessler DI. Can anesthetic technique for primary breast cancer surgery affect recurrence or metastasis? Anesthesiology. Oct 2006;105(4):660-664.
Myles PS, Peyton P, Silbert B, Hunt J, Rigg JR, Sessler DI. Perioperative epidural analgesia for major abdominal surgery for cancer and recurrence-free survival: randomised trial. BMJ. 2011;342:d1491.
Day A, Smith R, Jourdan I, Fawcett W, Scott M, Rockall T. Retrospective analysis of the effect of postoperative analgesia on survival in patients after laparoscopic resection of colorectal cancer. Br J Anaesth. Aug 2012;109(2):185-190.
Chen WK, Miao CH. The effect of anesthetic technique on survival in human cancers: a meta-analysis of retrospective and prospective studies. PloS one. 2013;8(2):e56540.
Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. May 13 2006;367(9522):1618-1625.
Kairaluoma PM, Bachmann MS, Rosenberg PH, Pere PJ. Preincisional paravertebral block reduces the prevalence of chronic pain after breast surgery. Anesth Analg. Sep 2006;103(3):703-708.
Schnabel A, Reichl SU, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of paravertebral blocks in breast surgery: a meta-analysis of randomized controlled trials. Br J Anaesth. Dec 2010;105(6):842-852.
Wildgaard K, Ravn J, Kehlet H. Chronic post-thoracotomy pain: a critical review of pathogenic mechanisms and strategies for prevention. Eur J Cardiothorac Surg. Jul 2009;36(1):170-180.
Neal JM, Brull R, Chan VW, et al. The ASRA evidence-based medicine assessment of ultrasound-guided regional anesthesia and pain medicine: Executive summary. Reg Anesth Pain Med. Mar-Apr 2010;35(2 Suppl):S1-9.
Neal JM. Ultrasound-guided regional anesthesia and patient safety: An evidence-based analysis. Reg Anesth Pain Med. Mar-Apr 2010;35(2 Suppl):S59-67.
Macario A, Vitez TS, Dunn B, McDonald T. Where are the costs in perioperative care? Analysis of hospital costs and charges for inpatient surgical care. Anesthesiology. Dec 1995;83(6):1138-1144.
Ilfeld BM, Mariano ER, Williams BA, Woodard JN, Macario A. Hospitalization costs of total knee arthroplasty with a continuous femoral nerve block provided only in the hospital versus on an ambulatory basis: a retrospective, case-control, cost-minimization analysis. Reg Anesth Pain Med. Jan-Feb 2007;32(1):46-54.
Jakobsen DH, Sonne E, Andreasen J, Kehlet H. Convalescence after colonic surgery with fast-track vs conventional care. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. Oct 2006;8(8):683-687.
I make checklists for everything. Whenever I go on a trip, I use the same packing checklist to make sure I don’t forget anything – umbrella, jacket, socks, snacks, passport, and a few other things. Using a checklist not only ensures that I bring everything I’m going to need on the trip; I’m convinced that it makes my packing ritual faster because I don’t have to keep going back and forth to my suitcase whenever I suddenly remember something I left out. Even our dog has her own packing checklist for trips to her sitter’s house. Now that my wife and I have 2 kids, the traveling checklist has gotten more complex and even more essential.
As an anesthesiologist, I believe that checklists are part of our culture whether we state them explicitly or not. When I first started my training as a new anesthesiology resident, I learned a mnemonic “MOM SAID” (although there are variations) to check and set up my anesthesia workstation before every case. Each letter stood for an important element of my preparation checklist: MachineOxygenMonitorsSuctionAirwayIVDrugs. I would then follow this mnemonic with reminders for myself; for example “MOM SAID, ‘don’t forget your stethoscope’” or “MOM SAID, ‘don’t forget to print a baseline EKG strip.’” Over the years, I have found modified forms of this same checklist to be useful just before and after induction, and I continue to use this method today.
Unfortunately, in the complex environment of surgery and perioperative medicine, there aren’t easy mnemonics for everything, and medical errors happen. The use of a formal checklist for surgical and invasive procedures that promotes interactive discussion among all team members and includes important steps related to the entire surgical episode has been promoted by the World Health Organization (WHO) as part of its global Safe Surgery Saves Lives campaign (http://www.who.int/patientsafety/safesurgery/en/). In the May 2014 issue of ASRA News, our Resident Section Committee article by Dr. Jennifer Bunch presents her experience implementing the WHO Surgical Safety Checklist abroad.
In regional anesthesiology and pain medicine, one of the most dreaded complications besides nerve injury and local anesthetic systemic toxicity (LAST) is the wrong-site block. The risk factors related to this medical error have been well-studied and include patient, physician, procedural, environmental, and system factors (1,2). Despite the best intentions, wrong-site blocks have not gone away (3-5). ASRA has been hard at work developing a standardized pre-procedure checklist for regional anesthesiology that has been published in Regional Anesthesia and Pain Medicine. ASRA’s recommended checklist includes the following elements: patient identification with assessment of pertinent medical history, separate verifications of the surgical procedure and block plan, confirmation that appropriate equipment and medications for the block procedure and resuscitation are immediately available, and a pre-procedural time-out. Dr. Mulroy was charged with heading this task force and has been kind enough to summarize ASRA’s checklist project in this issue of ASRA News.
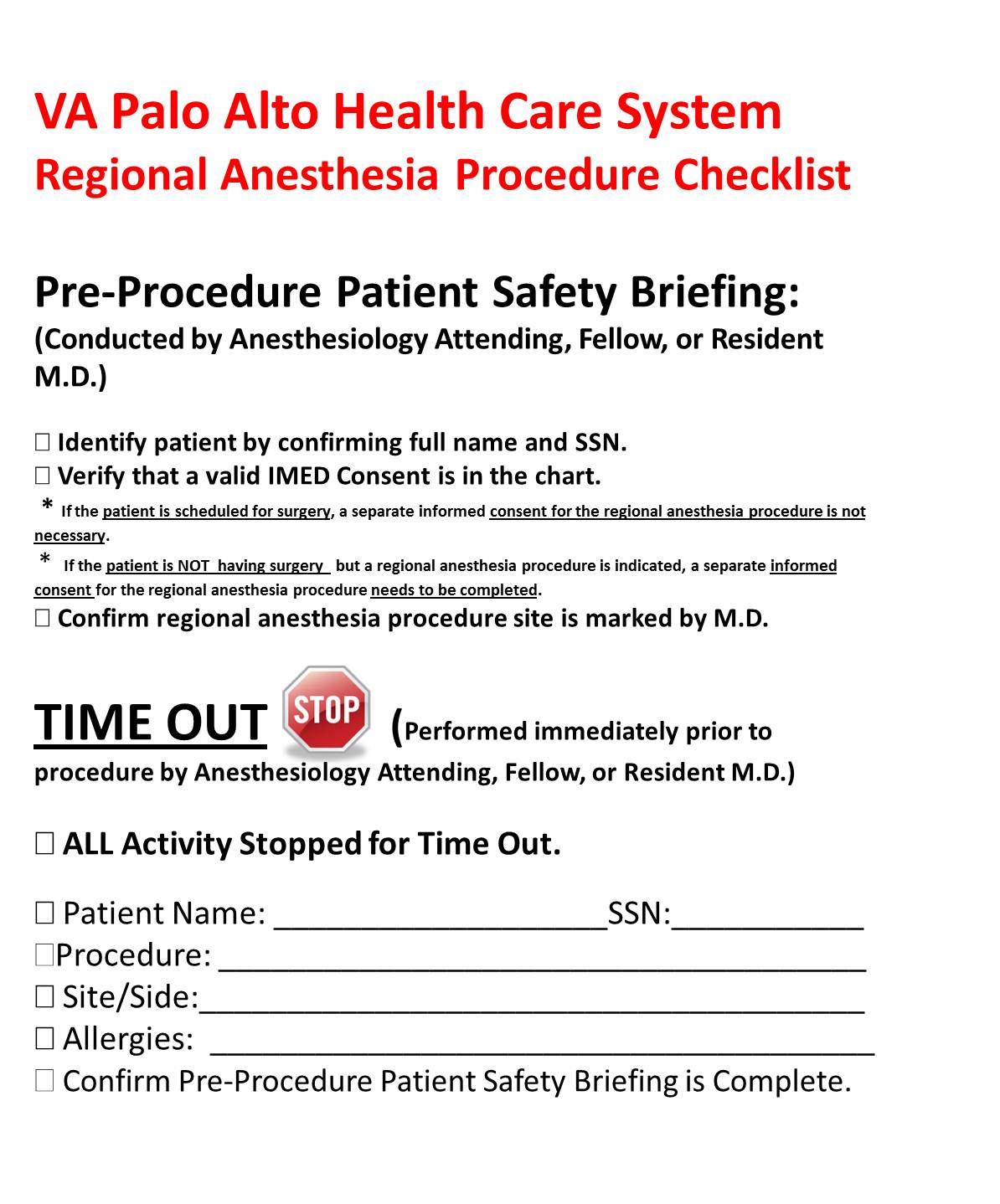
Figure 1. Pre-Block Time Out Cognitive Aid
With the publication of this checklist, ASRA is once again taking a stand in support of patient safety. The process of verifying the correct patient, correct site, and correct implants or devices for patients undergoing any invasive procedure, including peripheral nerve blockade, must be consistently and reliably applied for every patient. Since there is no easy mnemonic to help providers remember every step, and the order in which they must occur, I suggest using a standardized cognitive aid for block procedures (Figure 1) that should be posted in a consistent location visible to all providers involved in the procedure and in every location in which these procedures will occur. During the time-out process, it is essential that all team members involved in the patient’s procedure stop what they are doing and actively participate.
When I started my current job in 2010, the Veterans Health Administration (VHA) had just issued Directive 2010-023, “Ensuring Correct Surgery and Invasive Procedures,” and this VHA Directive was considered inclusive of regional anesthesia procedures. We have had a process similar to the ASRA checklist in place since then, and I acknowledge that implementing change is hard. Yes, following a checklist requires extra steps. Yes, it may even take more time. The bottom line is – it takes a lot more time, effort, and expense to deal with the complications that may result if you don’t do this. The ASRA checklist is not prescriptive and allows for local institutional interpretation and application. If I routinely use a checklist when I pack my suitcase, I can’t think of any good reason not to use one for the safety of my patients.
Cohen SP, Hayek SM, Datta S, Bajwa ZH, Larkin TM, Griffith S, Hobelmann G, Christo PJ, White R. Incidence and root cause analysis of wrong-site pain management procedures: a multicenter study. Anesthesiology. 2010 Mar;112(3):711-8.
Edmonds CR, Liguori GA, Stanton MA. Two cases of a wrong-site peripheral nerve block and a process to prevent this complication. Reg Anesth Pain Med. 2005 Jan-Feb;30(1):99-103.
Stanton MA, Tong-Ngork S, Liguori GA, Edmonds CR. A new approach to preanesthetic site verification after 2 cases of wrong site peripheral nerve blocks. Reg Anesth Pain Med. 2008 Mar-Apr;33(2):174-7.
Al-Nasser B. Unintentional side error for continuous sciatic nerve block at the popliteal fossa. Acta Anaesthesiol Belg. 2011;62(4):213-5.
Originally included in my editorial for the May 2013 issue of ASRA News.
In the May 2013 issue of ASRA News, I want to highlight a special Pro-Con feature dedicated to the controversial topic of regional anesthesia and analgesia in the patient at risk for acute compartment syndrome. I want to personally thank our surgical colleagues from the University of Alberta who were willing to write a thoughtful “Con” article for our newsletter. Before jumping to debate each of their points, we need to give them careful consideration. With the paucity of evidence-based recommendations on this topic, it is crucial to have an open honest dialogue between all members of the healthcare team. This Pro-Con is not meant to provide answers but to provide talking points for an ongoing conversation.
In my previous position at UCSD, we had a Level 1 trauma center where we would keep one operating room (OR) set up and warm at all times for the occasional direct-to-OR resuscitation. We saw all types of acute and subacute orthopedic trauma, and no two cases were approached the same way. Did I consider regional analgesia for each of these patients? Yes. Did I perform regional analgesia for all of them? No.
In order to have a meaningful discussion on this topic with our surgical colleagues, we must first be part of the conversation. In the specialty of Regional Anesthesia and Acute Pain Medicine, this means emphasizing more the “Acute Pain Medicine” part than the “Regional Anesthesia” part. The value that we bring to perioperative patient care must be more than just a set of interventional peripheral nerve and neuraxial block techniques. We have to know when these techniques are and are not indicated and have other modalities for analgesia at our disposal when providing consultation on complicated trauma patients. In addition, the service we provide cannot be time-limited. How can we say that superior pain control is only available from 7 am to 5 pm not including weekends and holidays?
When it comes down to it, managing patients at risk for compartment syndrome is tough. The benefits of analgesia have to be weighed with the potential for neurovascular compromise. Sometimes you will perform regional analgesic techniques for them; other times you won’t. Sometimes, you will place catheters that you can dose later when the risk profile improves; other times you may be consulted for help later in the hospital stay. Sometimes you will convince the surgeon to preemptively perform fasciotomies in a patient in whom you anticipate a difficult postoperative course. The context for this decision-making will vary from institution to institution, but ongoing communication with the surgical team is indispensible. Be a consultant; be available; and continue to be part of the conversation.
Edward R. Mariano, MD, MAS, FASA, FASRA is a physician specializing in anesthesiology, professor, husband, and father working to improve pain control, outcomes, and the overall experience for patients having surgery

 In order to accomplish this mission, we need the best information available to guide our decisions and a diversity of perspectives to enhance our ability to train new clinicians and explore relevant research questions. We have been fortunate to partner with our friends and colleagues in the Veteran and Family Advisory Council (VFAC) on a number of exciting projects. First, our Service manages the simulation center at VAPAHCS and is responsible for coordinating simulation-based training for all clinicians. Members of VFAC have been directly involved in simulation activities, even taking on active roles as the patient or family member in standardized training scenarios, to help us educate clinicians from various disciplines and all training levels. Debriefing after these simulation exercises gives our clinical trainees and practicing clinicians the unique perspective of real patients and family members which is essential to their professional development as modern medicine continues to progress towards a model of patient-centered care.
In order to accomplish this mission, we need the best information available to guide our decisions and a diversity of perspectives to enhance our ability to train new clinicians and explore relevant research questions. We have been fortunate to partner with our friends and colleagues in the Veteran and Family Advisory Council (VFAC) on a number of exciting projects. First, our Service manages the simulation center at VAPAHCS and is responsible for coordinating simulation-based training for all clinicians. Members of VFAC have been directly involved in simulation activities, even taking on active roles as the patient or family member in standardized training scenarios, to help us educate clinicians from various disciplines and all training levels. Debriefing after these simulation exercises gives our clinical trainees and practicing clinicians the unique perspective of real patients and family members which is essential to their professional development as modern medicine continues to progress towards a model of patient-centered care. Once a year, our Service organizes a faculty development retreat during which we reassess our mission, vision, strategic priorities, and tactics and work on one or two big ideas. Two years ago in 2015, we invited our VFAC partners to join us at our annual retreat to brainstorm improvement ideas related to patient-centered care in the perioperative environment, intensive care unit, and pain management. The general theme of the retreat addressed public perception and professional reputation of anesthesiologists and the specialty of anesthesiology. Having members of VFAC present at the retreat to share their knowledge, opinions, and questions has inspired a few subsequent improvement activities and other projects to enhance the range of services that we provide to our patients and their families.
Once a year, our Service organizes a faculty development retreat during which we reassess our mission, vision, strategic priorities, and tactics and work on one or two big ideas. Two years ago in 2015, we invited our VFAC partners to join us at our annual retreat to brainstorm improvement ideas related to patient-centered care in the perioperative environment, intensive care unit, and pain management. The general theme of the retreat addressed public perception and professional reputation of anesthesiologists and the specialty of anesthesiology. Having members of VFAC present at the retreat to share their knowledge, opinions, and questions has inspired a few subsequent improvement activities and other projects to enhance the range of services that we provide to our patients and their families. Many people, even those who work in the operating room every day, take safe anesthesia care for granted. There has been growing pressure recently to abandon the team model and remove physician anesthesiologists’ supervision of nurse anesthetists with the latest threat coming from within
Many people, even those who work in the operating room every day, take safe anesthesia care for granted. There has been growing pressure recently to abandon the team model and remove physician anesthesiologists’ supervision of nurse anesthetists with the latest threat coming from within  Healthcare around the world is changing. In the United States, healthcare reform has been focused on achieving the “triple aim” as described by Berwick (1). This
Healthcare around the world is changing. In the United States, healthcare reform has been focused on achieving the “triple aim” as described by Berwick (1). This  To date, anesthetic interventions focused on targeting acute pain have not demonstrated long-term functional benefits (12,13). Perhaps implementation of a PSH with better care coordination that includes individualized
To date, anesthetic interventions focused on targeting acute pain have not demonstrated long-term functional benefits (12,13). Perhaps implementation of a PSH with better care coordination that includes individualized 

 re administering a medication, it’s not enough just to understand the complex pharmacologic effects of the drug and determine the right dose. The anesthesiologist also has to know how to dilute and prepare the drug, the appropriate route for the medication, which other medications are and are not compatible, and how to program the infusion device. In addition, an anesthesiologist has to be technically skilled at finding veins—sometimes in the hand or arm, sometimes leading centrally to the heart—in order to give the medication in the first place.
re administering a medication, it’s not enough just to understand the complex pharmacologic effects of the drug and determine the right dose. The anesthesiologist also has to know how to dilute and prepare the drug, the appropriate route for the medication, which other medications are and are not compatible, and how to program the infusion device. In addition, an anesthesiologist has to be technically skilled at finding veins—sometimes in the hand or arm, sometimes leading centrally to the heart—in order to give the medication in the first place.