Guest authored by Jody C. Leng, MD, MS, and Kariem El-Boghdadly, MBBS, BSc (Hons), FRCA, EDRA, MSc. Dr. Leng is a Clinical Assistant Professor at Stanford University School of Medicine and is the Director of Regional Anesthesiology and Acute Pain Medicine at the Veterans Affairs Palo Alto Health Care System. Dr. El-Boghdadly is a consultant anaesthetist and the research and development lead for anaesthesia and perioperative medicine at Guy’s and St Thomas’ NHS Foundation Trust and is an honorary senior lecturer at King’s College in London.
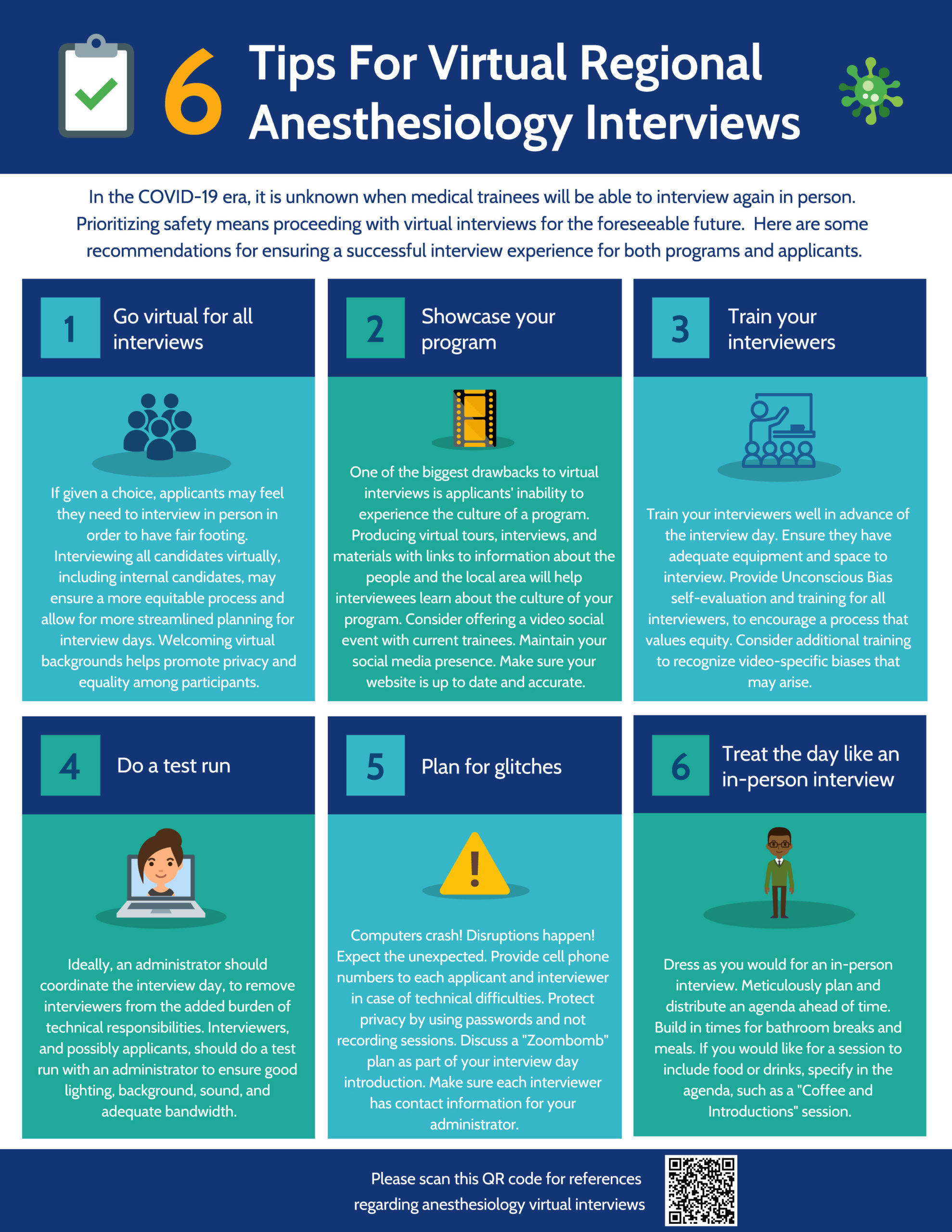
The Covid-19 pandemic has normalized virtual everything. For both interviewers and interviewees, participating in virtual interviews for subspecialty fellowship programs has required major adjustment. We have summarized some key lessons we have learned in preparing for our second year in a row of virtual regional anesthesiology and acute pain medicine fellowship interviews in the following infographic.
COVID-19 has changed every aspect of our personal and professional lives.
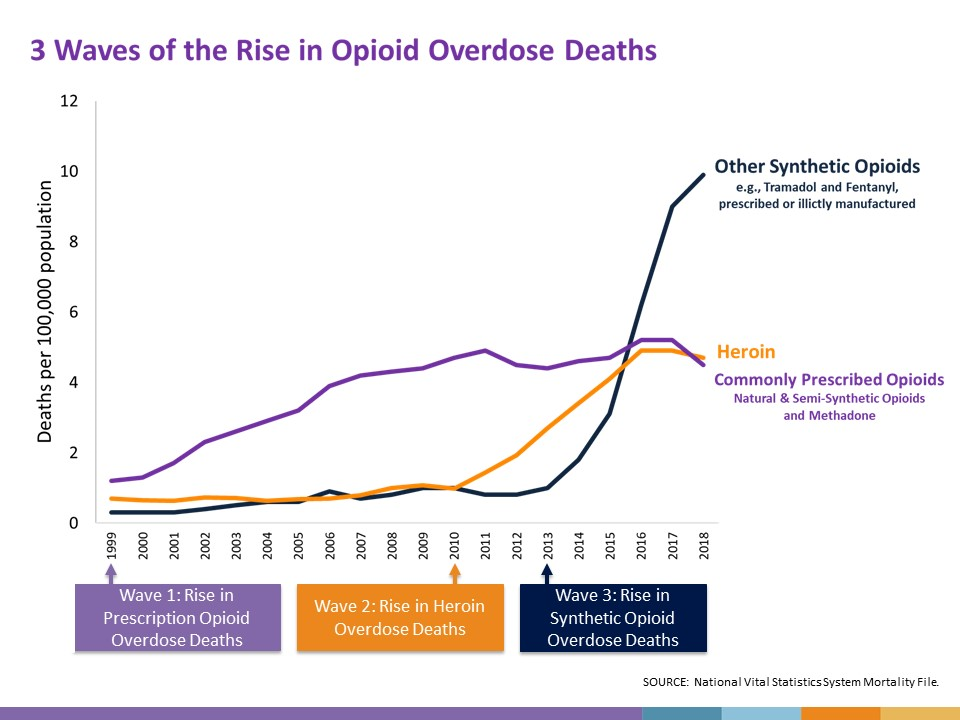
In the midst of this pandemic, we still have an opioid epidemic. It is not one thing unfortunately, and the Centers for Disease Control and Prevention (CDC) describe three distinct waves of opioid-related overdose deaths.
Given the complexity of the opioid epidemic, we have to keep working within our spheres of influence. For those of us in anesthesiology, that means focusing on surgical patients: improving their outcomes and providing effective perioperative pain management along with opioid stewardship.
Dr. Chad Brummett and his colleagues at Michigan OPEN have been leading the way in procedure-specific opioid prescribing recommendations. Their process, which takes into account data from the Collaborative Quality Initiative (CQI), published studies, and expert input, specifically focuses on the perioperative care of patients who are not taking any opioids prior to surgery.
Through multimodal analgesia, we prevent and treat pain in a variety of ways without depending solely on opioids.
At our institution, we offer patients regional anesthesia and have been able to decrease the amount of opioid pills that patients are given when they leave the hospital by basing the prescription on how much they use the prior day. Patients participate in this process, and we give them clear instructions on how to safety taper their opioids at home.
As a representative of the American Society of Anesthesiologists (ASA), I have been able to collaborate with surgical societies such as the American Society of Breast Surgeons and the American Academy of Orthopaedic Surgeons to develop pain management recommendations and toolkits that emphasize multimodal analgesia, use of regional anesthesia techniques for targeted non-opioid pain management when it is available, and opioid safety in the hospital and at home.
Despite the massive amount of resources, human effort, and time dedicated to the fight against COVID-19, we have still managed to make progress in decreasing opioid-related risk in the perioperative period. However, there is still a lot of work left to do, and our patients are depending on us.
At the end of July, we graduated three new physician experts in regional anesthesiology and acute pain medicine (RAAPM), and I could not be more proud of them! From our welcome party in the summer of 2019 to a year’s worth of teaching sessions, socials, and medical missions to the opening of the new Stanford hospital, the #COVID19 pandemic and #BlackLivesMatter movement – what a year for our amazing grads! Check out this fantastic graduation video from Dr. Jody Leng:
Our graduating fellows surprised me with the honor of being their Teacher of the Year along with Dr. Ryan Derby! It is such a privilege to be part of our fellows’ training every year and see them grow into physician consultants with RAAPM expertise.
Our new fellows are off to a strong start and are now officially part of our Stanford RAAPM family! If you are interested in learning more about our fellowship program, please visit our fellowship website and contact me with any questions.
2020 is a unique graduation year for all of our anesthesiology residents and fellows due to COVID-19, but never before has the role of anesthesiologists been more relevant. The American Society of Anesthesiologists (ASA) has prepared this special graduation message so programs can incorporate it into their virtual ceremonies, and it features a very special commencement speaker: Dr. Jerome Adams, the Surgeon General of the United States!
Nearly all of these physicians who are just starting their careers specializing in anesthesiology have completed 4 years of college, 4 years of medical school, and 4 years of internship and residency plus 1 or more years of fellowship training for many. Hopefully this message will help our newest graduates, their families and friends, and their teachers and mentors recognize and commemorate this important milestone in their lives.
Dealing with the COVID-19 pandemic information overload
Discussing hard topics on social media
Being a positive voice for marginalized groups
Being a “Chief Cheerleader”
The key to joy at work
In this episode of The Brave Enough Show, I had a chance to speak with host Dr. Sasha Shillcutt about a variety of topics including #HeforShe, leadership, and maintaining a positive voice on social media. Enjoy!
Many people, even those who work in the operating room every day, take safe anesthesia care for granted. There has been growing pressure during this pandemic to remove physician supervision of nurse anesthetists with the latest threat coming from within Veterans Affairs (VA) healthcare. For our Veterans, our heroes and arguably some of the most medically complex patients, having a physician in charge of anesthesia care at hospitals where anesthesiologists and nurse anesthetists work together as a team makes the most sense.
Having a team with members who train differently and have different perspectives can only benefit the patient; anesthesiologists are physicians who draw on their medical training while nurse anesthetists bring valuable nursing experience. If you were a patient having surgery, wouldn’t you want an anesthesiologist directly involved in your care and leading the anesthesia team? If the answer is yes, please send your comments to Safe VA Care and let your elected officials know by contacting them.
Providing anesthesia is often compared to flying a passenger airplane, and the anesthesia care team model is like having both a pilot and a co-pilot.
Who thinks flying has become so safe that we no longer need the pilot? Seconds count in flight, and they count just as much in the operating room when a patient’s life is on the line.
In 2016, the VA rejected independent practice for nurse anesthetists after careful consideration, but this decision was recently overturned by a memo citing the COVID-19 pandemic. This memo abolishes the anesthesia care team model without giving Veterans a choice. Veterans having surgery may only get a nurse anesthetist without the option of having an anesthesiologist involved. If they were given the choice, however, I think our Veterans would choose an anesthesiologist or an anesthesia care team led by an anesthesiologist instead of a nurse anesthetist alone. We all should. In areas affected by surges of COVID-19, elective surgeries at the VA are stopped so there is no shortage of anesthesiologists.
Anesthesiologists all over the world have been fighting COVID-19 and have shown what they can do with their specialized medical training in a crisis. Although commonly referred to as “going to sleep,” general anesthesia is more like a complex drug-induced coma that can carry serious risk. If or when a crisis happens during surgery, every patient should have access to an anesthesiologist.
Modern anesthesiologists are physicians first but also scientists, educators, and patient safety advocates. Anesthesiologists specialize in relieving anxiety, preventing and treating pain, preventing and managing complications related to surgery, critical care, and improving patient outcomes. The average anesthesiologist spends nearly a decade in postgraduate education after college including medical school and logs 16,000 hours of clinical training to learn to apply the best available evidence in clinical practice. Academic physicians and scientists focused on anesthesiology are responsible for the discovery of newer and safer anesthetics, pain therapies, and technologies that are advancing healthcare throughout the world.
Anesthesia administration by non-physicians such as nurse anesthetists and certified anesthesiologist assistants is supported by the American Society of Anesthesiologists within the physician-led anesthesia care team model. To uphold the highest quality physician-led anesthesia care for our nation’s Veterans, please speak up by supporting Safe VA Care and reaching out to legislators.
It only takes a minute to stand up for safety, but the consequences of not saying something may be serious and long-lasting.
Due to the COVID-19 pandemic, the usual spring meeting season for medical societies never got started. In San Francisco, all events hosting more than 1000 people were prohibited. As a result, the 2020 annual ASRA regional anesthesiology and acute pain medicine meeting was cancelled.
However, there were nearly 400 scientific abstract posters submitted to the meeting and posted online. For so many registered attendees, the ASRA meeting was an opportunity to share their latest research and medically challenging cases with their colleagues and solicit feedback.
There was no way to preserve the complex structure of an ASRA meeting (e.g., workshops, plenary lectures, problem-based learning discussion, networking sessions), but a moderated poster session was feasible using common videoconferencing applications. The Chair of the 2019 ASRA spring meeting, Dr. Raj Gupta, took it to the next level by using StreamYard to simultaneously broadcast the video feed to multiple social media platforms (e.g., Twitter/Periscope, Facebook, YouTube). In addition to accessing the livestream for free, participants could make comments and pose questions to the speakers and moderator through their social media applications.
Dr. Gupta hosted 6 sessions, and these were archived on YouTube for later viewing. As an example, here is one session focused on regional anesthesia abstracts in which I participated:
Although it was disappointing to not have an ASRA spring meeting this year, something good came out of it. The livestreamed poster discussions were an innovative way to showcase the science and educational cases as well as leverage social media to attract a global audience. Since medical conferences may never completely return to pre-COVID normal, embracing technology and incorporating online sessions should be considered by continuing medical education planners going forward.
Personal protective equipment (PPE) for personnel involved in advanced airway management in cases of known positive or suspected COVID-19 should not replacerecommendations by the Centers for Disease Control and Prevention (CDC).
However, the additional risk of exposure to healthcare personnel involved in advanced airway management for a disease with airborne transmission must be taken into consideration. Past experiences with variations in PPE during other major respiratory diseases in recent history have been published along with recommendations for the current COVID-19 pandemic. Experts have recommended a higher level of PPE for personnel involved in advanced airway management due to limitations of standard PPE, particularly neck and wrist exposure.
https://t.co/Rz7z2U9Ycp This was an important study demonstrating potential for contamination of exposed areas when using typical enhanced PPE (contact/droplet/airborne). As we all get prepared for #2019NCoV, what are people doing to mitigate this risk? pic.twitter.com/CMSeWMYcpl
Use of an air filtration system, preferably an N95 mask, is recommended by CDC and anesthesia societies and is a minimum requirement for airway management personnel. Proper air filtration is a basic need for healthcare professionals caring for patients with airborne diseases and participating in aerosol-generating procedures (AGPs). N95 fit testing should be prioritized for these healthcare professionals. For airway management personnel who do not successfully fit test or cannot wear an N95 for other reasons, ideally a hooded Powered Air Purifying Respirator (PAPR) should serve as the alternative.
Implementation of these features will vary given the variability of available PPE between institutions and supply shortages worldwide. It is essential to train airway management staff as soon as possible to develop a local PPE protocol that takes into account CDC and special precautions for high-risk procedures like intubation as described above. Each facility will likely develop its own unique PPE protocol.
The following videos are being shared for educational purposes only. They represent only one example of applying additional precautions to PPE for airway management personnel, and there will be many others. Creating local videos can help expand training at a facility without depleting available PPE supplies. Remember that each institution or practice will develop its own version of PPE for airway management personnel, and many variations can achieve the same goal.
Traffic is non-existent. Schools are closed. Restaurants are only offering take-out and delivery. Parking lots at strip malls are empty on weekends. Only a limited number of people at a time are allowed inside the grocery store.
Welcome to the post-normal era since the COVID-19 pandemic hit the scene in Northern California.
One day we will look back at this time and realize how much it changed everything. Simple things like a handshake or sitting together with a colleague during a lunch break will hopefully never be taken for granted again
The California Governor has issued a statewide order to shelter in place. It’s only natural that the husband and father parts of me consider staying home like everyone else.
But I’m not like everyone else, and none of us in healthcare are. We are considered “essential,” which is why we continue to go to work day-and-night while the rest of our society shelters in place in a monumental effort to “flatten the curve” of COVID-19.
I have always liked this blog by Dr. Kathy Hughes about working at hospitals around the holidays and being essential. Hospitals at that time of the year are actually festive places. It’s different now. There are no holiday potlucks in the ward lounges to bring people together. There is no celebrating. Yet, we all understand that we are needed and share the burden of being essential together.
Our work as anesthesiologists has changed. We no longer perform elective surgeries in our operating rooms. The weight of our role as specialized physicians has shifted from perioperative and pain medicine to emergency response, critical care, and crisis management. We are at particularly high risk since COVID-19 is a respiratory disease. Every time we are called to perform tracheal intubation in an infected or suspected patient who is coughing and having trouble breathing, we are staring down the barrel of a gun.
Protecting ourselves is a priority because our expertise is a limited resource. If we get sick, we can’t help others, and we risk spreading COVID-19 to our families. Personal protective equipment or PPE is a necessity, and multiple layers are required by anesthesiologists and other airway management personnel given the high risk procedures we do in these patients. It takes time to put on PPE, but there can be no shortcuts when it comes to safety. SLOW IS SAFE, and we need to remember that there are no more emergency intubations in this post-normal era.
To all airway management personnel:
❗This is the post-normal era. There are NO MORE emergency intubations.
❗Proper donning of PPE takes time. SLOW = SAFE.
❗You are a precious resource. Do not risk getting exposed.
Being essential in the hospital is not limited to just the healthcare professionals of course. The engineers, the technicians, the housekeepers, the cafeteria and food service workers–they are the unsung heroes of the hospital during this pandemic. Without them, our facilities and our healthcare workers would cease to function. Whenever I see them, I thank them for the work they are doing to support us on the front lines of patient care. We share stories of how things used to be and give each other some encouraging words.
It is surreal to get up, get ready for work, have a cup of coffee as part of my normal morning routine, drive through deserted streets, and walk into the hospital not knowing what the day will bring. We have a job to do, and that calling to help humanity drives us to keep coming to work. We chose medicine, but medicine chose us too.
Edward R. Mariano, MD, MAS, FASA, FASRA is a physician specializing in anesthesiology, professor, husband, and father working to improve pain control, outcomes, and the overall experience for patients having surgery